What kind of diseases are dysarthria and anarthria? Dysarthria is a violation of the pronunciation side of speech, which is caused by insufficient innervation of the speech apparatus. With dysarthria, the pronunciation of sounds and the prosodic aspect of speech (voice strength, tempo, rhythm, intonation) are impaired. Speech disorder is associated with organic damage to the central and peripheral nervous systems. Anarthria is the absence of speech caused by damage to the neuromuscular system, which provides its articulatory component, that is, the correction of pronounced sounds and words using the tongue, pharynx, cheeks and teeth. Patients suffering from anarthria understand the role they hear. Diagnosis and differential dysarthria with other disorders of speech function are carried out by doctors and speech therapists at the Yusupov Hospital.
Using modern neuroimaging methods, the location of the lesion that caused dysarthria is determined in the brain. The patient is examined using the latest equipment from leading global manufacturers. Patients are treated by a multidisciplinary team of highly qualified specialists. Early diagnosis of a speech disorder and an individual approach to the treatment of each patient make it possible to quickly restore impaired speech in patients who have suffered a stroke, traumatic brain injury or suffer from diseases of the nervous system.
general description
Dyslalia refers to various speech defects that are observed in people with normally developed articular apparatus and unimpaired hearing. The diagnosis of speech impairment (dyslalia) is made on the basis of a speech therapy examination of the patient. Sometimes the help of related specialists is required - an otolaryngologist, a neurologist, a dentist. Treatment of dyslalia is complex and includes several stages.
Complications
If you do not seek help in time, then more serious problems will arise in the future, which will provoke the appearance of other speech defects. The disturbances also affect communication with others: people have difficulty understanding the speech of a dysleptic.
At school age, peers may ridicule and imitate the child. And this will already affect mental health.
Motor dyslalia can lead to errors in writing (dictation, composition, presentation) and reading. Because of this, there is poor performance in school in humanities subjects. Only a competent speech therapist can eliminate and correct speech.
Types of dyslalia
The following main forms of dyslalia are distinguished:
- simple - the patient pronounces one group of sounds incorrectly;
- complex dyslalia - the patient incorrectly pronounces two or more groups of sounds; this type of disease is also called polymorphic dyslalia.
For convenience, various pronunciation disorders are formed into groups, each of which is designated by a term derived from one of the Greek letters.
Thus, they distinguish:
- rhotacism - the patient has problems with the letter r;
- hitism - problems with the letter x;
- Lambdacism - problems with the letter l;
- kappacism - problems pronouncing the letter k;
- sigmatism - problems with whistling and hissing sounds;
- gammacism - the patient has trouble pronouncing the letter g;
- Yotacism - problems with the letter y.
Depending on the causes, the following types of disease are distinguished:
1. Mechanical dyslalia.
2. Functional dyslalia. Caused by a disorder of the brain or the influence of various social factors on the child. There are several subtypes of this form of the disease:
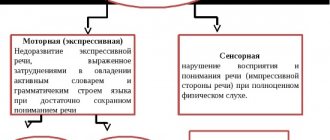
- sensory functional dyslalia - the patient has no problems with the articular apparatus, the cause of the pathology is defects in the development of the hearing and speech centers;
- motor functional dyslalia - caused by problems with the articular apparatus, due to which a person cannot pronounce certain sounds correctly.
Sometimes a mixed sensorimotor form of the disease is observed.
In some cases, speech impairment is normal. It is associated with age-related characteristics of speech perception by ear and disappears independently after reaching 5 years.
Disadvantages of pronunciation of individual sounds
| Defective sound | Phonetic defect (sound distortion) | Phonemic defect (confusion, sound replacement) | ||
| Name of pronunciation defect | Types of defective pronunciation | Name of pronunciation defect | Types of substitutions | |
| Sound R | Rotacism | Velar, uvular, lateral, buccal, single-impact, “coachman” | Pararotacism | Р = Р' Р = Л' Р = J Р = Г Р =Д |
| Sound L Sound L' | Lambdacism | Bilabial, softened | Paralambdacism | L = Y L = G L = L' L = R |
| Sounds S, S' Sounds Z, Z' Sound C | Sigmatism | Interdental, labial-dental, lateral, subdental, sibilant | Parasigmatism | S, Z, C = W S, Z, C = F S, Z, C = T S, Z, C = Shch S - W; C = H |
| Sound Ш Sound Ж Sound Ш Sound Ш | Sigmatism | Mesdental, buccal, lateral, “lower”, posterior lingual, softened, shortened, affricative | Parasigmatism | Sh, Zh, Shch = T Sh, Zh, Shch = F Zh = Sh Zh = Z Shch = S' Sh = Shch Ch = T'; Ch = Sh' |
| Sound j | Yotacism | Soft lower and upper articulation | Paraiotacism | J = L' |
| Sounds K, K | Kappacism | Vocal, laryngeal | Paracapacism | K = T |
| Sounds G, G | Gammacism | Fricative velar, pharyngeal | Paragammatism | G = T |
| Sounds X, X | Hitism | Vocal, laryngeal | Parachytism | |
Causes of dyslalia
All possible causes of dyslalia in children can be divided into two large groups:
- Socio-biological. It is known that young children largely copy the behavior and speech of adults and try to imitate them. If parents lisp with a child or communicate little with him, do not pay attention to how his oral speech develops, then over time this can lead to the development of speech defects.
- Organic. Disturbances in sound pronunciation in dyslalia are caused by a violation of the structure of the speech apparatus. Any such problem can cause the development of speech defects in dyslalia.
In preschool children, the disease may be caused by age-related factors. In this case, speech defects go away on their own after some time and do not require special treatment.
However, it is imperative to pay attention to how the child speaks. Indeed, if uncontrolled, physiological dyslalia can eventually develop into a pathological form, which requires specialized speech therapy treatment.
In addition, it is at a young age that a child develops communication skills that will play an extremely important role throughout his life.
How can you tell if your child has dyslalia?
The following signs indicate that the baby has developed dyslalia:
- he misses sounds, and in any part of the word;
- some sounds are replaced by similar ones in place or method of formation;
- the child pronounces the word in a distorted form, even if he has known it for a long time and well.
The rest of the child's speech is correct. He uses cases, plural and singular forms, gender endings without errors, and is not confused in the meaning of well-known words.
Diagnosis of dyslalia
Diagnostics is complex and includes the following main stages:
- Anamnesis collection. The doctor conducts a survey of the patient and his parents. The specialist is interested in whether the mother had any problems during pregnancy (threat of miscarriage, infectious diseases, etc.), how the birth took place (whether it was natural or a cesarean section, whether the child received head injuries during childbirth or immediately after it, and etc).
- Studying the patient's medical record. The doctor studies what diseases the baby has suffered, and whether there are any pathologies among them that can lead to the development of speech disorders.
- Various tests, during which the specialist determines the level of development of speech, psychomotor skills, and musculoskeletal system of the patient.
- Assessment of the level of development of the child’s speech apparatus.
In addition to speech, the specialist uses additional materials during diagnosis.
If the cause of a child’s speech impairment is organic disorders of the speech apparatus, then in addition to the speech therapist, other specialists (dentist, orthodontist) should also participate in the process of diagnosis and treatment. In addition, the child may need to be examined by a neurologist and surgeon. If during the examination the patient was diagnosed with hearing loss, then an examination by an otolaryngologist is necessary.
Definition and classification
Functional dyslalia is a speech disorder without articulatory defects, manifested by distortion or inaccuracy of word reproduction. Dyslalia can be simple - monomorphic, when the child cannot pronounce one sound or sounds from one group; polymorphic - complex when the pronunciation of several sounds from different groups is disrupted. The formation of lexical and grammatical speech does not suffer.
Functional dyslalia is divided on the basis of pathogenesis: motor (lack of readiness of the organs of articulation to perform complex movements), sensory (difficulty in recognizing and distinguishing similar sounds) and mixed, when both mechanisms are affected simultaneously.
Experts also identify several forms of this speech disorder:
- Articulatory-phonemic - characterized by the replacement of some sounds with a similar one. For example, “chicken-kuricha”, “cat-koska”, etc.
- Acoustic-phonemic - develops with poorly formed hearing, when children cannot correctly recognize the acoustic characteristics of sounds. In such cases, the words look like this: “bark-mountain”, “nora-time”.
- Articulatory-phonetic – distortion of some letters (“p”, “sh”), etc.
Often children develop not just one form of the disease, but a mixed version of it. In this case, there is a substitution of sounds, a violation of the hardness and softening of words, insufficient pronunciation of letters: “th”, “k”, “r”, “x”, etc.
Treatment of dyslalia
Before moving on to methods for eliminating dyslalia, it is necessary to determine the reasons that led to the patient’s speech disorder.
Correction of dyslalia of mechanical origin takes place in several stages. First, the patient undergoes surgery, during which anatomical defects that interfere with normal speech are eliminated.
Most often, such an operation is necessary for adults after receiving severe injuries to the jaws and other organs that make up the speech apparatus.
If the organic form of the disease cannot be cured by surgery, then speech therapy for dyslalia is necessary.
| Correction of dyslalia |
In this case, the patient works with a speech therapist, performing special corrective exercises to normalize speech. The most difficult thing to treat is complex dyslalia in children, in which the child cannot correctly pronounce 4 or more groups of sounds.
With this form of the disease, the child’s phonemic hearing is usually impaired, so treatment is primarily aimed at improving the ability to distinguish and perceive sounds. After this goal is achieved, speech correction begins.
It is very important that not only the speech therapist, but also the parents work with the child. Correct speech should be heard in the house. There is no need to repeat after the child his incorrect pronunciation. On the contrary, you should draw his attention to errors in speech and teach the baby to pronounce words correctly.
Since dyslalia includes many different speech defects, the correction exercises will be different.
Exercises in the treatment of dyslalia are aimed at developing the speech apparatus. For this purpose, the following techniques can be used:
- exercises to develop fine motor skills;
- speech therapy massage;
- increased hearing sensitivity;
- teaching your child the basics of proper breathing.
When the child masters certain general speech skills, the speech therapist begins targeted correction aimed at teaching the child the correct pronunciation of certain sounds with which he has certain problems.
To achieve these goals, various speech therapy techniques have been developed. It is advisable to organize activities in a playful way so that the child does not lose interest in them. The doctor and the child play, talk, read books, sing songs, learn poems, and so on.
It is very important that dyslalia correction classes are conducted on a regular basis (at least 2-3 times a week). In addition, the child must study at home, completing the tasks given to him by the specialist. The duration of therapy depends on the severity of dyslalia and lasts on average from one month to six months. For adults, this period can be significantly shorter, since it is much easier for them to follow all the recommendations of a speech therapist.
| Stages of speech therapy for dyslalia |
Article:
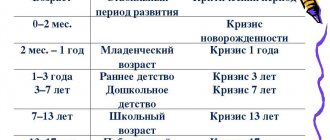
With the comprehensive development of a child, it is first of all necessary to pay attention to the child’s formation of correct and competent speech.
Undoubtedly, already in preschool age a child has a need to communicate with others. At this age, the first foundations of literate speech are laid. However, already at this stage of development the child may experience difficulties. The main task of parents at this age is to promptly contact specialists who can competently help the child overcome any speech difficulties that have arisen. A child’s speech is formed gradually, by imitating the pronunciation of the sound complexes of the people around him. The child masters correct sound pronunciation through the reproduction of intermediate sounds. This period is called physiological tongue-tiedness. The process of speech formation is directly related to the mental development of the child. Accordingly, any speech deviations may indicate features of the development of certain mental functions.
First of all, it is necessary that the child develops correct sound pronunciation. It includes the phonetic design of speech and a complex of speech motor skills, such as speech breathing, reproduction of sounds and their combinations, voice formation, stress in words, as well as intonation of phrases.
When the pronunciation side of speech is violated, defects in phonetic speech formation are formed. Experts call dyslalia one of the most common and mildest speech development defects. With dyslalia, the child does not pronounce some sounds and may distort them or replace them with other sounds. Such speech difficulties can make it difficult to communicate with others and can also lead to other developmental problems in the child. In this regard, timely identification and correction of such sound pronunciation disorders is necessary. These examinations can be carried out comprehensively with the presence of various specialists, and the speech therapist teacher also has the right to independently conduct research into the characteristics of a child with dyslalia.
General ideas about dyslalia
Dyslalia is a violation of sound pronunciation with normal hearing and intact innervation of the speech apparatus.
This disorder usually manifests itself in features of the reproduction of speech sounds, such as distortion during pronunciation, replacement of one sound with another, failure to pronounce any sound, as well as mixing of sounds.
The term “dyslalia” was first introduced by Vilnius University professor, doctor I. Frank. In his monograph in 1827, he used the term for the generalized meaning of pronunciation disorders of various etiologies. The Swiss doctor R. Schulthess in the 30s of the 19th century divided all speech disorders into stuttering and tongue-tiedness. At the same time, he designated tongue-tiedness with the term “dyslalia”, in a narrower meaning than that of I. Frank. R. Schulthess classified only pronunciation disorders caused by anatomical defects in the organ of articulation.
Working on his classification of speech disorders, Kussmaul took Schulthess's point of view as a basis. He called all speech defects formed due to disorders in letter sound formation as tongue-tied. Two variants of tongue-tiedness were also identified and described: congenital and acquired. The latter occurs due to improper upbringing and lack of exercise. In this case, congenital or organic tongue-tiedness is one of the forms of central speech disorder.
With the development of speech therapy science, the concept of “dyslalia” was clarified, and the features of violations of the sound aspect of speech and the mechanisms underlying them were identified. This is reflected in the works of such authors as Berkan, Gutzman, E.S. Borishpolsky, T.B. Filicheva and L.G. Volkova.
Causes of dyslalia
Speech impairment is a fairly common phenomenon not only among children, but also among adults. Accordingly, the occurrence of such features is different. However, they may be the result of untimely or ineffective treatment. Children may experience disturbances in sound pronunciation, phonetics and phonemics, and the construction of agrammatic phrases.
Dyslalia is a violation of the pronunciation side of speech with intact innervation of the speech apparatus, which most often manifests itself in childhood.
There are several causes of speech disorders: organic and functional.
Organic causes of dyslalia include congenital or acquired defects in the bone and muscle structure of the peripheral part of the speech apparatus.
- Disadvantages of the structure of the maxillodental system:
- dental defects;
- defects in the structure of the jaw;
- features of the frenulum of the tongue.
- features of the size and shape of the tongue.
- irregular structure of the hard or soft palate. With such structural features, first of all, difficulties arise in pronouncing hissing and whistling sounds.
- unique structure of the lips. With such features, it is difficult to pronounce labial, labial-dental, and vowel sounds.
The functional prerequisites for the occurrence of dyslalia include unfavorable heredity, a difficult situation in the intrauterine development of the fetus, childbirth itself, as well as Rh conflict between mother and child.
The social situation of the development of a preschool child also influences the formation of competent speech development. An unfavorable social situation may exist in the family and in the surrounding society. Usually, the following preconditions for the formation of speech characteristics are identified: maternal deprivation, the presence of speech characteristics in one of the family members, as well as a stressful situation experienced.
Forms of dyslalia
B.M. Grigshpun identified three forms of dyslalia: acoustic-phonemic, articulatory-phonemic and articulatory-phonetic.
Acoustic-phonemic dyslalia.
With acoustic-phonemic dyslalia, difficulties in the formation of speech with sounds are revealed, formed in the process of selective processing of phonemes according to their acoustic parameters in the sensory link of the speech perception mechanism. Such operations include identification, recognition, comparison of acoustic characteristics of sounds and decision-making about the phoneme.
With such a defect, the immaturity of phonemic hearing is identified, through which recognition and distinction of phonemes in words occurs. The child cannot recognize any acoustic feature of a complex sound by which one phoneme is opposed to another. Accordingly, phonemes are replaced based on the similarity of common features. As a result, the sound is identified incorrectly. Such features make it difficult for both the speaker and the listener to correctly understand speech.
With acoustic-phonemic dyslalia, the child does not have hearing impairment. The defect boils down to the fact that he does not selectively develop the function of auditory discrimination of certain phonemes.
Articulatory-phonemic dyslalia.
This form includes defects caused by the immaturity of the operations of selecting phonemes according to their articulatory parameters in the motor part of speech production. There are two main types of violations. In the first case, the articulatory base is found to be incompletely formed and reduced. When selecting phonemes, instead of the required sound (which is absent in the child), a sound that is close to it in terms of a set of articulatory characteristics is selected. In this case, the phenomenon of substitution, or replacement of one sound with another, is observed. A sound of simpler articulation acts as a substitute.
With this disorder, the articulatory base is fully formed. There has been a process of complete mastery of all articulatory positions necessary for the production of sounds, but when selecting sounds, an incorrect decision is made, as a result of which the sound appearance of the word becomes unstable (the child can pronounce words correctly or incorrectly). This leads to confusion of sounds due to their insufficient differentiation, and to their unjustified use.
Substitutions and confusions in this form of dyslalia are realized on the basis of the articulatory proximity of sounds. These phenomena are noticed primarily between sounds or classes of sounds that differ in one of the characteristics: whistling and hissing, between noisy plosives, anterior-lingual and posterior-lingual.
With this form of dyslalia, the child’s phonemic perception is most often fully developed. The child can distinguish all phonemes and understands words, including paronymous words. The child understands his defect and tries to cope with it. In many cases, such self-correction under the control of auditory control is learned successfully.
Defective pronunciation in this form of dyslalia is determined not by motor impairments themselves, but by a violation of the operations of selecting phonemes based on their articulatory characteristics. The child copes with tasks of imitation of complex non-speech sounds, which require certain structures of the speech organs for their implementation; sounds that are more complex in motor terms are often made and replaces with them the missing sounds that are the simplest in articulation.
Articulatory-phonetic dyslalia.
This form includes defects in the sound design of speech caused by incorrectly formed articulatory positions.
Sounds are pronounced abnormally, distorted for the phonetic system of a given language, which is formed in a child with this form of dyslalia, but phonemes are realized in unusual variants (allophones). Most often, the erroneous sound is close in its acoustic effect to the correct one. The listener, without much difficulty, correlates this variant of pronunciation with a specific phoneme.
There is another type of distortion in which the sound is not recognizable. In such cases they speak of omission, emission of sound. The case of skipping sounds with this form of dyslalia is a rare phenomenon (more often occurs with other, more severe defects, for example, with alalia). With dyslalia, an analogue of sound, purely individual in its acoustic effect, performs the same phonemic function in the child’s speech system as the normalized sound.
Not all sounds are affected: for example, with various individual characteristics of pronunciation, the acoustic effect when pronouncing labial (plosive and sonorant) consonants, as well as anterior lingual plosives and sonorant consonants, turns out to be within normal limits.
The main group of sounds in which distorted pronunciation is noted are the front-lingual non-plosive consonants. Less common is defective pronunciation of posterior lingual plosives and midlingual consonants.
In the course of mastering pronunciation skills, the child, with the help of his hearing, gradually gropes for those articulatory positions that correspond to an adequate acoustic effect. The child remembers these positions and repeats them in the future as needed. When mastering the correct patterns, the child must learn to distinguish between patterns that are similar in the pronunciation of sounds, and develop a set of speech movements necessary to reproduce sounds.
Depending on how many sounds are pronounced defectively, dyslalia is divided into simple and complex.
Simple (monomorphic) include disorders in which one sound or sounds of homogeneous articulation are pronounced defectively; complex (polymorphic) include disorders in which sounds of different groups are pronounced defectively.
An integrated approach to the examination of children with dyslalia
The main goal of examining a child with possible dyslalia is to make an accurate speech therapy diagnosis, which is necessary for further selection of an adequate method of helping a particular child. In this regard, he identifies five main tasks of speech therapy examination:
- Distinguish dyslalia from other speech features.
- Identification of the characteristics of the defect, whether it is independent or included in a particular system complex.
- Identification of all defectively pronounced sounds.
- Identification of the root cause of sound pronunciation disorders.
- Determining whether there are secondary developmental features associated with a defect in sound pronunciation.
The examination of a child with dyslalia should be carried out by a psychological, medical and pedagogical commission, which includes: speech therapist, psychologist, orthodontist, neurologist, ENT, psychiatrist. With such a set of specialists, it will be possible to comprehensively examine the picture of the child’s development, give an expanded conclusion about his maturation, clarify ways to correct the disorder and make a forecast for the future formation of speech development.
The examination of a child with a speech disorder may include various sections. First of all, the child’s early developmental history is identified, then the correct pronunciation of all speech sounds is checked using a variety of aids, then the structural features of the speech apparatus are studied, as well as the identification of auditory differentiation. The diagnosis reveals the child’s vocabulary and grammatical structure of speech. Writing characteristics are examined in school-age children, since dyslalia can lead to difficulties in mastering writing.
Speech therapy examination of a child with dyslalia
When a large number of specialists are present at the commission, the speech therapist examines only the characteristics of the child’s speech, without studying the developmental history or structural features of the speech apparatus. In the absence of all specialists, the speech therapist himself carries out the entire examination procedure.
There are several options for speech examination cards for children with dyslalia. Let's look at one of them, since it is more complete and adapted to the work of a teacher - speech therapist. L.G. Volkova developed examination schemes for children with various speech disorders in the form of forms.
Scheme of examination of children with dyslalia L.G. Volkova
Personal data Last name, first name of the child Date of birth (day, month, year) Date of examination (day, month, year) Age (number of years, months) Home address, telephone number Which children's educational institution he came from (number, district) Date of admission to the speech therapy group (date, number of the protocol of the medical-psychological-pedagogical commissions, from what date)
diagnosis of the district (city) medical-psychological-pedagogical commission
Information about parents Mother: Full name, profession, education, place of work (or not working) Father: Full name, profession, education, place of work (or not working) Complaints from parents (features of the child’s behavior; unusual , from the point of view of parents, actions; disturbances in speech, communication; learning difficulties: in kindergarten or at school; the impact of sound pronunciation disorders on the assimilation of the program in kindergarten or on the success of school; difficulties in contact with peers and adults: acquaintances and strangers) Hereditary diseases (presence of speech disorders, neuropsychic, chronic diseases in parents and relatives) General anamnesis Which pregnancy is the child from?
Nature of pregnancy: toxicosis, chronic and infectious diseases Childbirth: rapid, protracted, dehydrated
Features of early development: Past diseases: up to 1 year from 1 to 3 years Infections Somatic diseases Data on speech development Nature of sound babble. Time of appearance of phrasal speech.
Speech therapy examination State of sound pronunciation. Determining the nature of the violation of consonant sounds: absence, replacement with other sounds, defective articulation in various pronunciation conditions: • in isolation - by imitation of a speech therapist; • in open, closed syllables with confluence; • in words: one-syllable, two-syllable and three-syllable, simple syllabic structure, consisting of open syllables; the same thing in complex words: with closed syllables and with a combination of consonants; • in phrases rich in the sound being tested; • in coherent speech - nursery rhymes, poems, texts.
Features of the dynamic side of speech
- pace: normal, accelerated, slow; • rhythm: normal, arrhythmia, correct use of pauses in the flow of speech; • intonation (use of the main types of intonation): narrative, interrogative, incentive.
Anatomical structure of the articulatory apparatus • lips: thick, thin, shortened upper lip, incomplete closure of the lips; • jaws: progenia (excessive protrusion of the lower jaw), prognathia (excessive protrusion of the upper jaw); • bite: open anterior, open lateral; • teeth: small, excessively large front teeth, absence, supernumerary, outside the jaw arch, etc.; • tongue: too thick, does not fit in the mouth, too narrow, shortened hyoid ligament; • palate (hard, soft): excessively low hard palate, flattened, “Gothic”, dome-shaped; shortened soft palate, bifurcation of the small uvula. State of facial motor skills - raise eyebrows up - lower; frown - peace; close your eyes - open; squint; puff out your cheeks - peace; reflect on the face facial poses “joy”, “sadness”, “suspicion”, “surprise”, “anger”; - according to the verbal instructions of the speech therapist, show how a person eats sour lemon, sweet candy, bitter onion, pickled cucumber. Upon completion of the tasks, it is noted: facial expressions are intact; amimicity; insufficient mobility of individual facial muscles (forehead, eyes, cheeks, lips). State of oral praxis Kinesthetic basis of speech: the ability to perform individual articulatory movements.
The kinetic basis of speech is for the lips: stretch your lips forward - smile at peace; raise the upper lip up - lower the lower lip down - lower the upper lip down, raise the lower lip up; for the tongue: open your mouth - show a wide tongue - raise it to the upper lip - lower it to the lower lip - put it in your mouth - close your mouth; open your mouth - show your narrow tongue; touch the right and left corners of your mouth with your narrow tongue; put your tongue in your mouth - close your mouth; open your mouth - show alternately wide and narrow tongue; open your mouth - run a narrow tongue around the upper and lower lips in a clockwise direction, then in the opposite direction - put your tongue in your mouth - close your mouth; - for the lower jaw: carefully move the lower jaw to the right - to the left; - for the soft palate: open your mouth - put your tongue on your lower lip - cough with your mouth open and your tongue on your lower lip. Visually: the muscles of the soft palate contract and lift it. Upon completion of the tasks, the following should be noted: range of movements (full - all movements are completed; incomplete - part of the movements is completed; range of movements is impaired - a series of movements is distorted or movements are omitted); accuracy of execution (preserved - all movements are performed in a given sequence; impaired - search for articulation or additional movements); tone (preserved - movements are performed with the necessary strength and tension; impaired - movements or part of the movements are performed sluggishly, without sufficient tension of the articulatory muscles); tempo of movements (normal - one movement is performed after another without pauses; slow - there are pauses of 3-5 seconds between individual movements; accelerated - movements are performed so quickly that the previous movement has not yet been completed, but the subject is already beginning to perform the subsequent movement) ; synkinesis (no; yes - when performing the exercise, additional movements appear in both articulatory and facial muscles). State of auditory, respiratory and voice functions. Write out data on the state of biological hearing from the medical record or refer the child for a consultation with an otorhinolaryngologist. Check the state of speech perception during a conversation with the child and when performing instructions such as “Take the doll”, “Put the doll in the crib” , “Go to the closet and take the cubes”, “Collect a pyramid.” When examining the state of respiratory and vocal functions, the following should be noted: type of breathing (thoracic, diaphragmatic, abdominal, mixed); volume, duration of speech exhalation: for children 5 years old for 2-3 words, for children 6-7 years old for 3-5 words per exhalation. Describe the voice according to the following parameters: voice strength (normal, loud, excessively quiet), pitch (low voice, high, mixed, normal), timbre (monotonous voice, presence or absence of a nasal horn). State of phonemic analysis, synthesis and phonemic representations Simple (elementary) phonemic analysis When examining the state of these functions, the speech therapist takes into account the conditions for sound isolation (according to N. Kh. Shvachkin): stressed vowels are distinguished more easily than unstressed vowels at the beginning of a word; fricative consonants stand out more easily from the beginning of a word; plosive consonants are more easily distinguished from the end of a word; hard consonants stand out more easily than soft ones; The sound [P], as a longer sound, stands out more easily at the beginning of a word. p—it is most difficult for children to determine the presence of a vowel and isolate it from the end of a word, since the vowel sound is perceived by the child not as an independent sound, but as a sign of a consonant sound (V.K. Orfinskaya). Isolating a sound against the background of a word. Instructions: “Do you hear the sound [M] in the word HOME? Do YOU hear the [K] sound in the word MAC?” etc. Isolating the initial stressed vowel sound from a word. Instructions: “What sound do you hear in the word ANYA? OLYA? MORNING? IRA? Echo? What sound do you hear in the word MAC? MOUTH? What sound do you hear in the word GARDEN? STUTTERER? FUR COAT? BUG? PIKE? FATHER? BALL? PAW? CANCER? The speech therapist pronounces the sound necessary for isolation with intonation, i.e., highlighting it with his voice. Differentiation of sounds by contrasts Venya - Fenya; mouse - bear; horns - spoons; dot - daughter; duck - fishing rod; ears - snakes. Saika – bunny; injection - angle; mask - Masha; shawl - sorry; bowl - bear; bow - hatch. Kol - goal; gang - seagull; juice - clack Complex phonemic analysis Determining the place of a sound in a word (globally first: at the beginning, at the end, in the middle) Instructions: “(Where is the sound [S] in the word GARDEN?, in the word FOCUS?, in the word FOX?” Then more precisely: “What place is the sound [C) in the word SANI?, in the word WASP?, in the word NOSE?” The child’s answers: “In the word SA-SANI, the sound [C] comes first; in the word OSA on the second; in the word NOS in third place.” The speech therapist pronounces the sound [C] intoned in an isolated position and as part of words. Determining the sequence of sounds in a word. Instructions: “What sound do you hear at the beginning of the word SSSANI? Child’s answer: “Sound [S].” “Correctly, what sound do you hear after the sound [S]? SAAANI" The child's answer is "Sound [A]." “What sound do you hear after the sound [A]? SANNY" child's answer: "Sound [N]." “What sound do you hear after the sound [N]? SANIIII." Child’s answer: “Sound [I].” Thus, the speech therapist intonately pronounces the sound that the child must identify. The speech therapist can pronounce the sounds of another word offered to the child in a slightly less intonated manner if the child correctly determines the sequence of sounds in the first word. Determining the number of sounds in a word.
Instructions: “How many sounds are in the word MAK? in the word FLOUR? in the word Lump? These words consist of sounds that are preserved in children's pronunciation. They are formed in early ontogenesis on the basis of unconditional reflex reactions of sucking, swallowing, and chewing. Then the child is asked to determine the number of sounds in the words that the child pronounces incorrectly, for example, in the words: JUICE, BRACE, SOCK; NOISE, MICE, HAT; CANCER, CORA, MARKET, etc. The principle of selecting words proposed for quantitative phonemic analysis is that if a word contains a sound that is complex in articulatory and acoustic characteristics, for example, [S], [SH], [R ], etc., then the remaining sounds of the word should be simple in this regard. Phonemic synthesis The speech therapist invites the child to compose words from sounds given in the normal sequence: [C], {A), [D]; [HOUSE]; [HAND]; [P], [O], [H], [K], [A]. Next, the speech therapist invites the child to compose words from sounds given in a broken sequence: [M], [O], [S]; [O], [L], [B]; [U], [W], [A], [B]; [A], [M], [P], [K], [A]. Phonemic representations The child is asked to choose a word for a given sound. Instructions: “Name a word with the sound [S], [3], [C], [Sh], [Zh], [H], [Sh], [L], [R].” From the different pictures proposed by the speech therapist, the child is asked to select those whose names contain this sound. For example, for the sound [S]: airplane, glass, cheese, bag, pine. Features of vocabulary Study of nominative vocabulary The speech therapist finds out the child’s knowledge of words from the following groups: toys, clothes, shoes, dishes, furniture, vegetables, fruits, household items, pets, wild animals, plants, school supplies, transport, pictures of nature. Next, the child is asked to name the object according to its description. Instructions: “What is the name of the object in which soup is cooked?” Child’s answer: “Pan,” or “What is the name of the object used to dig the ground?” - “Shovel.” Then knowledge of generalizing words for the above groups is established; ability to select synonyms for a group of words.
Selection of antonyms.
Words that can be offered to children: WET, SOFT, SHARP, THIN, DILIGENT, SMART, TIMID, MUDDY, CALM, etc. Study of predicative vocabulary The child names actions based on the presented object: pike - swims, snake - ..., swallow - ..., grasshopper. The child names the depicted objects with their characteristic actions. The child names words denoting the cries of animals and birds: domestic ones - moos, neighs, grunts, barks, growls, meows, cackles, crows, cackles, quacks, etc.; wild - howls, yelps, growls, snorts, croaks, croaks, chirps, croaks, chirps, etc. Object pictures are used. The child names the actions of people of various professions: painter - paints, tailor ... (sewing), doctor ... (treats), hairdresser ... (cuts), blacksmith ... (forges), pilot ... (flies), tractor driver ... (plows). Study of the grammatical structure of speech Study of the ability of inflection Change by case. Instructions: “I have a doll. I don't have... (doll). ^ I sing a song... (to the doll). I'm bathing (the doll). I like to play with... (doll). I dream of a beautiful (doll).” Conversion of nouns in the nominative singular case into the plural: table - tables, hand - -..., leaf - .,, window -.... Formation of singular and plural genitive nouns: House - houses - houses; window - windows - windows; wood - ... - .., brand - ... - ; Apple - … - … ; table - … - ; ball—…—-…; book - … ; cherry - … - . Agreement of adjectives with singular nouns in gender. Object pictures are used. Sample: ball - red, cup - red, dress - red. Then the task: Scarf (green), hat - ..., coat - Study of word formation ability Formation of a noun with diminutive suffixes. Pictures with images of objects of different sizes are offered: chair - (high chair) spoon - (spoon) bed - (crib) doll - (doll) picture - (picture) house - (house) Formation of adjectives from nouns (preparatory group). Words for presentation: wood - wooden, rubber - ..., glass - ..., crystal - ..., leather - iron - ..., silk - ..., paper - ..., lace Formation of verbs of motion using prefixes (preparatory group). Words for presentation: walk - go out - enter - enter - go - go around - go away - pass - go - go; run - ...; fly …; swim - ...; go Next, the speech therapist finds out whether the pronunciation defects have been eliminated (where, how many, results), and writes an updated diagnosis or speech therapy report.
In this diagnosis, the author takes a comprehensive approach to the study of dyslalia. An anamnesis of the child’s development, the state of his sound pronunciation, structural features of the speech apparatus, speech motor skills, the state of auditory function, the state of respiratory and vocal function, features of the dynamic side of speech, the state of phonemic analysis, synthesis and phonemic representations, features of vocabulary, as well as the grammatical structure of speech are revealed. .
Such a comprehensive study of the characteristics of a child with dyslalia contributes to the development of an adequate and timely system of assistance.
Based on the diagnostic results, a diagnostic card is filled out and a conclusion is written. Usually, the speech therapy report notes the form of dyslalia, and also indicates the extent of sound pronunciation disorders, all sounds that the child pronounces defectively and the nature of their violation.
Conclusion
Dyslalia is a violation of the spoken aspect of speech with intact innervation of the speech apparatus, which often manifests itself in childhood.
There are two main forms of dyslalia: functional and mechanical. These forms depend on the location of the violations and the causes, the occurrence of a defect in sound pronunciation. With mechanical dyslalia, the peripheral part of the speech apparatus is disrupted. With functional dyslalia, organic disorders are detected.
There are three forms of functional dyslalia:
Acoustics – phonemic. In which phonemic or auditory perception is impaired.
Articulatory - phonemic. With this form, sounds are replaced or mixed.
Articulatory - phonemic. This form includes defects in the sound design of speech, formed on the basis of an incorrect speech family position.
To identify dyslalia, specialists use a diagnostic examination, which includes collecting anamnestic data on the child’s development, studying the structure of the speech apparatus and the speech examination itself. For the convenience of diagnostics, it is customary to use diagrams or forms of speech therapy examinations.
After the diagnosis, recommendations are made for further assistance in the development of the child or adult.
Bibliography
- Gorodilova V.I. and Rau E.F. Correction of deficiencies in the pronunciation of schoolchildren / Manual for teachers and speech therapists - M: 1952.
- Speech therapy: Textbook. for students defectol. fak. ped. higher textbook institutions / Ed. L.S. Volkova, S.N. Shakhovskaya. — M.: Humanite. ed. VLADOS center, 1998.
- Volkova G.L. Psychological and speech therapy study of children with speech disorders. Book publishing house "Saima". 1993
- Fundamentals of speech therapy // Ed. T.V. Volosovets. M., 2000.
- Fundamentals of the theory and practice of speech therapy / Ed. R.E. Levina - M., 1968.
- Essays on pathology of speech and voice / Ed. S.S. Lyapidevsky. - M., 1963.
- Paramonova L.G. Speech therapy for everyone. - St. Petersburg: Peter, 2004.
- Pravdina O.V. Speech therapy. 2nd ed. M., 1973.
- Rau F.F. Techniques for correcting deficiencies in the pronunciation of phonemes // Fundamentals of the theory and practice of speech therapy. M., 1968.
- Speech disorders in children and adolescents / Ed. S.S. Lyapidevsky. - M.: 1963.
- Filicheva T.B. Cheveleva N.A. Chirkina G.V. Fundamentals of speech therapy - M.; 1989.
- Khvattsev M.E. Speech therapy - M., 1959.
Diagnostic measures
To make a correct diagnosis and differentiate organic from functional pathology, consultations with several specialists are necessary - a pediatric neurologist, speech therapist, psychologist, otolaryngologist and pediatrician. At the appointment, the doctor uses the following diagnostic approaches:
- Collection of complaints and history of speech disorders. Parents are asked in detail when speech difficulties began, what they were accompanied by, whether the child has diseases of the nervous system, how the mother’s pregnancy proceeded, etc.
- Examination of the oral cavity.
- Study of the child’s speech skills: performing special exercises - opening and closing the mouth, stretching the lips into a tube, smiling, changing the positions of the tongue (wide, narrow, pipe). During such manipulations, the doctor notes the muscle tone of the articulatory apparatus and can identify its disorders.
- Assessment of sound pronunciation - the child is asked to name the objects shown in the pictures. The tasks are selected in such a way that the presented sound is in different positions - the beginning, end or middle of the word. After completing the study, you can find out the nature of the defect - omission, replacement, distortion or confusion of sounds.
- The speech therapist analyzes phonemic hearing - repeating syllables after a specialist, reading syllables from images.
- Additional instrumental diagnostic methods are electroencephalography, magnetic resonance imaging of the brain if organic pathology is suspected.
After completing the diagnosis, specialists make a diagnosis and prescribe the necessary treatment individually for each child.
Prevention
Preventive measures include monitoring correct pronunciation at home, helping the child develop speech, following the recommendations of a speech therapist and other specialists, a nutritious diet and an active lifestyle. If problems with speech are identified, parents should immediately contact a speech therapist and pediatrician, and not wait for them to be corrected on their own.
Functional dyslalia is not an organic pathology associated with damage to brain structures. In this regard, the speech therapy and medical measures used make it possible to restore speech development and achieve correct, literate speech.
The occurrence of pathology
With functional dyslalia, there is no structural damage to the brain or articulatory apparatus. The child hears normally. The environment in which the baby grows and disturbances in the neurodynamic processes of maturation of the cerebral cortex play a major role in the formation of the defect. Pathogenesis is explained by an imbalance or weakness of nervous processes in the central nervous system. An imbalance of excitatory and inhibitory processes may be located in Broca's center, and then a disturbance in the reproduction of words and sounds occurs; or in Wernicke's area, in this case the perception of sounds becomes difficult and the child replaces letters with similar sounds.
Provoking factors that can lead to pathology:
- poor physical health of the child;
- frequent colds and infectious diseases;
- hypo- and vitamin deficiencies;
- eating disorders (dystrophies);
- “lisping” with children of preschool and older age, leading to improper formation of speech centers;
- the child’s assimilation of adult speech defects (burr, incorrect pronunciation of words);
- bilingualism in the family, with children transferring sounds characteristic of one language to another;
- late contact with a speech therapist;
- unfavorable family environment, frequent stress;
- impaired mobility of the tongue, lips or lower jaw as a result of congenital or acquired defects;
- pedagogical neglect, in which adults do not communicate with the child and do not correct incorrect pronunciation, etc.
In addition, the occurrence of functional dyslalia can be influenced by the presence of delayed speech or mental development in various pathologies of the nervous system. In this case, treatment of speech disorders requires a long-term and comprehensive approach.