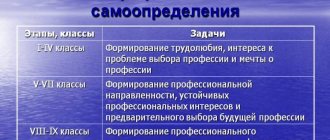
Neuroses in preschool children are a fairly common phenomenon, and they do not necessarily have to be preceded by some catastrophic event. Many parents, even very loving ones, do not attach importance to changes in their child’s condition and their behavior, and meanwhile the child’s neurosis is becoming stronger. Therefore, it is very important to promptly notice the symptoms of childhood neurosis and begin its treatment.
Symptoms
Based on the following signs, one can suspect that a preschool child has begun to develop neurosis:
- Emotional instability, frequent mood swings, reaching extremes: from laughter to tears.
- Increased irritability and excitability.
- Excessive vulnerability and touchiness.
- Frequent tantrums for no particular reason.
- Development of fears and phobias.
- Depressed state.
- Clearly increased discomfort, the feeling of which the child demonstrates when exposed to a certain type of irritant: for example, bright light, odors, temperature changes, sharp sounds.
- Problems with concentration, concentration, memory.
- Excessive, unfocused motor activity (in other words, fidgetiness).
- Inability to perform the same action for a long enough time (even playing your favorite game or watching your favorite cartoon).
- Problems with eating behavior (this can be either loss of appetite or “gluttony” that is unusual for a child before).
- Sleep problems (the child may have difficulty falling asleep or waking up, getting up frequently at night, may have nightmares, and may have problems with urinary incontinence while sleeping).
- Headaches, abdominal pain, pain in the heart area.
- Rapid fatigue during physical activity, general weakness.
- Tics, convulsions, muscle spasms, coordination problems.
If your child exhibits at least a few of the symptoms listed above, then this is a reason to contact a specialist.
Causes of childhood neuroses
In preschool children, neuroses can develop for reasons belonging to two main groups: physiological and psychological. Accordingly, the former are associated with the peculiarities of the functioning of the body of a particular child, and the latter – with the situation in the family, in the team (in kindergarten or school), with experienced stress, etc.
Physiological factors
- Heredity.
- Features of pregnancy and childbirth.
- Acute illnesses and chronic illnesses.
- Incorrect daily routine, insufficient sleep, poor nutrition, excessive workload in clubs and classes.
Psychological causes of neurosis in preschool children
- Problems in relationships with parents and other relatives (lack of attention or excessive severity; frequent quarrels between mother and father that occur in front of the child; likelihood of divorce; serious illnesses in parents that the child knows about; different attitudes of parents towards the child and his brothers/ sisters).
- Problems in relationships with peers in any group of which the child is a part (in kindergarten, in any club, on the playground).
- Problems in relationships with educators/teachers.
- Lack of self-confidence, low self-esteem, poor communication skills, increased anxiety.
A factor contributing to the emergence of childhood neurosis may be one specific event that caused him severe stress. This event does not have to be truly significant from the perspective of an adult - what matters is how the child himself perceives it.
Neurotic disorders in childhood and adolescence
Neuroses are diseases that can affect almost any initially mentally healthy child. Child psychiatrists distinguish between different diseases and conditions, which are collectively called “childhood nervousness.” There are neurotic reactions that occur in children to extremely strong stimuli, as well as astheno-neurotic reactions that occur against the background of a somatically weakened state. Neuroses are more persistent disorders and are systemic in nature. Neurotic reactions and neuroses may be accompanied by functional disorders of the central nervous system: tics, stuttering, enuresis, encopresis.
The etiology of these conditions is complex; constitutional and genetic factors are of great importance. In particular, twin methods show high concordance in identical twins (H. Remschmidt, 2001) compared to fraternal twins. Secondly, children and adolescents with neurotic disorders, compared to healthy children, are more excitable and less capable of adaptation; often such children have a high level of intellectual development and are endowed with talent (reader on child pathopsychology). Residual cerebral organic failure is also important. It can be caused by severe pathology, mainly in the second half of pregnancy, exposure to toxic substances (including alcohol), viral infections, Rh incompatibility, and so on. Pathogenic factors can be premature birth or prematurity. A frustrating traumatic situation plays a decisive role in the development of neurotic states. This situation, interacting with the individual psychological characteristics of the child (increased vulnerability, timidity, indecisiveness, shyness, social withdrawal, higher excitability or, conversely, inhibition) acts like a “key to the lock” and leads to anxiety, which is channeled into a symptom. Situations that can provoke anxiety and thus generate a neurotic state are diverse; they can be short-term, acute and chronic.
Frequent manifestations of nervousness in childhood include neuropathy - nervous weakness, which gradually decreases with age if favorable conditions are created for this in the family. Neuropathies in a child immediately after birth are manifested by frequent startlings from noise and restless sleep. By the age of one year, the manifestations of neuropathy become clearly expressed and remain so for the next few years. They are manifested by: an increased tendency to anxiety against the background of heightened emotional sensitivity and lability, easy fatigue, general nervous intolerance, poor tolerance to noise, stuffiness and bright light, sleep disturbances in the form of its superficiality, sensitivity or, on the contrary, deep sleep with involuntary urination, difficulty falling asleep , reduced need for daytime sleep, headaches, dizziness, vomiting, spasms (in particular laryngospasm), sweating, chills, somatic weakness.
Childhood neurosis is a psychogenic disease of a developing personality, that is, a disease that affects significant aspects of personality formation, the system of its relationships, first of all, relationships in the family and then relationships with peers and other adults. Neurosis occurs after a mental shock caused by a real or imagined threat to the life of a child or people close to him. Neurosis does not begin suddenly, but develops over a more or less long time, during which neuropsychic tension accumulates and does not receive its resolution. With neurosis, the psychogenic situation always “sounds” in the child’s experiences and is reflected in the emerging neurotic symptoms.
When intractable circumstances are resolved, neurotic symptoms tend to decrease. However, a child’s neurotic conditions can also lead to a delay in his mental development.
As mentioned above, frequent pathogenic situations for children and adolescents are situations of family interaction: the family atmosphere, the attitude of parents towards each other (disrespect, scandals, alcohol abuse by parents, fights), parental education style (excessive and or unstable demands on the child, abandonment, emotional coldness of parents and so on). Among school situations, the most common are: conflicts with peers, rivalry, harassment from older students, inadequate relationships from teachers, assessment situations, for example, an exam.
Common to all clinical forms of neuroses are a state of restlessness, anxiety and disorders of autonomic regulation. Psychomotor disturbances, represented by tics, stuttering, enuresis, can also occur with any neurosis. Each form of neurosis has its own central conflict.
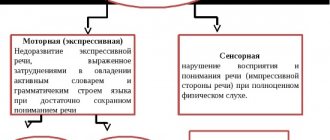
With neurasthenia , increased mental fatigue, distractibility and difficulty concentrating, combined with irritable weakness (incontinence of emotions and their rapid exhaustion), general lethargy and lack of stamina predominate. With neurasthenia, the peculiarity of a traumatic situation is that the needs on the part of the parents are not coordinated with the child’s capabilities. He cannot, despite his desire, assert himself in some areas or aspects of relationships that are significant to him; a conflict of self-affirmation manifests itself.
Phobic of fears, a high level of anxiety and self-doubt. A child with fear neurosis is not able to protect himself, his “I” from internal and external threats. This is a conflict of self-determination - self-confidence, the strength of one’s developing “I” when faced with imaginary or real dangers.
Obsessive neurosis is characterized by obsessive fears, thoughts and actions that occur, in addition to desire, often in the presence of constant doubts and hesitations in decision-making. Obsessive neurosis is determined by a moral, ethical or moral conflict - the presence of any incompatible feelings and desires in the child’s psyche. For example, a boy's desire to be like his father may clash with the father's rude attitude towards his mother, to whom the child is emotionally attached. Feelings of duty and love, which form sexual desires and prohibition, may be incompatible.
In hysterical neurosis , mood disorders, capriciousness, selfishness, and fixation of the attention of others on one’s painful state come to the fore. Hysterical neurosis implies a conflict between subjectively inflated desires and the possibilities of their real satisfaction. Most often, the conflict is caused by external obstacles to the realization of the acute need for love and recognition or dominance in relationships with others, their subjugation. In order to receive love and compensate for lack of attention, a child may complain of causeless malaise, inexplicable pain and long-gone fears.
The listed conflicts complement each other and cover the entire spectrum of conflict relations of the emerging personality. Common to all types of conflicts is the presence of an external obstacle to the expression of feelings and desires, the inability or impossibility of resolving it on one’s own, and the resulting tension and anxiety. It should be emphasized that we are talking about an internal, permanently occurring and individually manifested conflict, which is not always detected externally, psychologically with the “naked” eye and which is fundamentally different from open confrontation.
Fears . Being afraid is a natural, healthy reaction not only for a child, but also for an adult. However, fear, fear of something, should be distinguished from pathological fear, the criteria of which are: excessive intensity of fear, unusual content and unusual objects that cause fear, inadequacy of the fear reaction to the situation in which it arose, chronicity of fear and limitation of social activity due to fear , the impossibility of overcoming it. Preschoolers are often afraid of animals, fairy-tale characters, strangers; there are also fears of the dark, falling asleep, fire, fire, and fears of punishment by parents. By the age of 6-7 years, the fear of death reaches a high intensity. The fear of dying is an age-related reflection of the emerging concept of life, its starting point is birth, the mystery of which is comprehended in general terms by the beginning of senior preschool age, and the end is death, the awareness of inevitability, which comes for the first time and is manifested by the corresponding fear. The fear of death can be indicated by other fears associated with it: sleep, attack, fire, fire, fear of getting sick (in girls), fear of the elements (in boys). By the age of 8, children are already more afraid of the death of their parents. At school age, fears are less pronounced than in preschool age, but they are more associated with the social situation. During the school period, social fear begins - social phobia. The intensity of fears is related to the characteristics of the family situation. They are higher in families where they quarrel more, are strict with the child, or where parents are more worried about the child’s condition. In the latter case, the channel for transmitting fear is the mother's care.
Enuresis . The leading factor in enuresis is neuropathy, the determining role in which is played by sleep disturbances (restless sleep combined with motor restlessness). Excessive sleep depth is a compensatory inhibition that occurs in response to increased fatigue or excitability during the day. The dysontogenetic factor of enuresis is the unevenness of the child’s psychomotor development: slow/fast pace of development and stiffness/quickness of movements. A special role in the formation of enuresis is played by stress that arises due to the incompatibility of the temperaments of parents and children (a phlegmatic, slow child in a fast mother, for example). The aggravating factor of enuresis is family and household in the form of a lack of care and love, lack of parental feelings, lack of understanding of psychological factors in the mental development of the child.
Encopresis - fecal incontinence can begin at any age, most often at 5 years, and is often combined with enuresis. There are similarities in factors between these two disorders. Fecal incontinence is most often observed during the day, during play, walking, when the child’s natural urge is suppressed. Atrophy of urge gradually develops, children become insensitive to it and to the smell of feces. Complete atrophy of urge is observed in children whose fathers abuse alcohol, as well as in children with severe debilitating diseases of the gastrointestinal tract (dyspepsia, dysentery, constipation).
Stuttering . The determining role in stuttering is played by the constitutional factor, or speech, motor and communication insufficiency common to the parents. There may also be a general lack of motor skills, stiffness, tension, and excitability. In the process of speech development, children may find it difficult to translate internal speech into external speech; they understand more than they can say, and show silence and taciturnity. A psychologically traumatic factor can be forced communication, a large number of adults, placement in a nursery, or separation from parents. Another - dysontogenetic - factor is disturbances in the rate of speech development, its unevenness. This unevenness may be a reflection of the unevenness of general mental development. In general, stuttering in neuroses is characterized by: the emergence after a fright of excitement and tension, dependence in its course on the action of psychological factors, resumption in an environment that revives psychotrauma, mostly spasmodic (and not convulsive as in organic disorders) nature of the difficulties, inhibition at the beginning of a conversation , especially when communicating outside the family, with an unstable situational flow.
Types of deviation
There are quite a few types of neuroses, which are most common in preschool children:
- Anxiety neurosis. It may be associated with some kind of irrational phobia (for example, fear of the dark), or with a fairly adequate fear (for example, with the fear of being abandoned). The most striking example is the child’s reluctance to go to bed, the need for a night light, an open door, despite which he still sometimes wakes up screaming.
- Neurotic stuttering. This is a rather specific form of neurosis, and stuttering can either be permanent or manifest itself in the most exciting moments for the child. Boys suffer from this problem more often than girls.
- Neurotic enuresis. This is uncontrolled urination that occurs during sleep. It may be accompanied by general irritability and tearfulness, nervous tics, and stuttering.
- Neurotic tics. A tic is an obsessive movement that can involve quite different muscle groups, and which the child has little control over. So, this may be rapid blinking of the eyes; scratching the same place (even though it doesn't actually itch); movements around the neck, reminiscent of an attempt to loosen a tight collar; head shaking; rapid breathing, frequent coughing, “growling,” “groaning.”
- Hysterical neurosis. It is expressed in frequent seizures, hysterics, and attempts to attract increased attention to oneself. All this is usually connected with the fact that the child feels bad, but he does not know why and does not understand how to fix it.
- Asthenic neurosis. This form of the disease involves increased weakness and fatigue, lethargy, and indifference of the child.
- Depressive neurosis. Children with this neurosis are usually withdrawn, depressed, and uncommunicative. They tend to see the worst in every situation and predict the least successful outcome of any event.
These are just some of the most common forms - the manifestation of neurosis in each individual child may deviate from this list.
Types of teenage neuroses and their symptoms
The nature of the manifestations of neuroses in adolescents can be physiological and psychological.
Physiological symptoms:
- headaches and dizziness (due to spasms of cerebral vessels);
- sleep disorders (insomnia, nightmares, interrupted sleep);
- changes in appetite (up to neurotic anorexia or, conversely, bulimia);
- muscle weakness, increased fatigue;
- convulsions and nervous tics;
- neurotic cough;
- pain in the heart and stomach.
Psychological symptoms of neuroses:
- frequent mood swings, irritability;
- slight vulnerability, increased vulnerability, severe sensitivity;
- hysterical reactions;
- tendency to depression;
- various phobias (fears).
Depending on the clinical manifestations and combination of symptoms, the following types of neuroses are distinguished in adolescents:
- Hysterical neurosis, the manifestation of which is frequent hysterics with sobs. Hysterical paralysis of the limbs, loss of voice, vomiting, fainting, pseudoalgic manifestations (complaints of pain in the absence of organic damage) and others may be observed.
- Asthenic neurosis, the symptoms of which are general weakness, fatigue, sleep disturbances, manifestations of VSD in a teenager.
- Depressive neurosis with a desire for solitude, depressed mood. Often its development is associated with a stressful situation: parental divorce, death of a loved one, orphanhood and the role of “Cinderella”. Such neurosis can also occur if a teenager has a physical disability. Poor facial expressions, sad facial expressions, quiet speech, tearfulness, poor appetite and sleep, low self-esteem, low school performance - a portrait of a teenager with depressive neurosis.
- Obsessive-compulsive neurosis, manifested by tics, muscle spasms, and convulsions. In some adolescents, neurosis may manifest itself as an obsessive desire to utter indecent words. A neurotic compulsion can be dangerous (for example, a child may have a desire to jump from a balcony).
- Phobic neurosis, which is characterized by various fears (loneliness, death, darkness, etc.). Fear can occur in the form of an attack, especially before bedtime, accompanied by a feeling of anxiety, obsessive thoughts and ideas. It could also be a fear of giving an oral response in class or a fear of speaking in front of an audience.
- Hypochondriacal neurosis is manifested by excessive concerns and unreasonable fears of infection or the occurrence of various diseases.
How are neuroses treated in preschool children?
The first two specialists you need to contact if you suspect your child has a neurosis are a psychologist and a neurologist (able to establish, respectively, either psychological or neurological causes of the disease). Subsequently, they may refer the child to other, more highly specialized doctors (for example, an endocrinologist, cardiologist, psychiatrist). Do not be afraid to contact any of these specialists, since they are the ones who will help return your child to a healthy and comfortable state.
In addition, there are some preventive measures you can take yourself. So, it doesn’t hurt to teach your child to follow the correct daily routine, eat healthy food, exercise regularly, but not overwork in class. It is also important to improve the psychological atmosphere in the family, to let the son/daughter understand that he/she is loved and supported. This will not solve the problem at its root, but will help alleviate the child’s condition.
I like 2
Neurosis Child neurosis Pediatrics Pediatrician Health Child health Psychology Child psychology Psychological problems
Related Posts
leave a comment
Only 1 comment.
Alina
with us 2 years, 10 months, 12 days, 1 order made
2019-11-29 15:20:20My daughter was going through a difficult period now, a long and difficult adaptation to the garden since this fall, hysterics, tearfulness, waking up screaming at night and eventually began to sleep with us, although she had been sleeping well in her room since she was a year old. I started giving her vitamins Baby Bear Formula Calm, it had a very positive effect on the well-being and condition of our girl, she relaxed right before our eyes, smiles a lot again, and returned to her crib, although she now comes running to us sometimes, but not in tears, but simply hug. ,