What is the difference between anorexia and bulimia?
Anorexia is an eating disorder in which a person is perceived as fat even if they are within the normal body weight range.
This obsession with weight causes them to see their body incorrectly and motivates them to take extreme measures to lose weight, even using bulimia.
Bulimia is an eating disorder in which a person consumes food, usually high in calories, and immediately turns to resources to prevent weight gain. They may resort to, among other things, induction of vomiting, laxatives and diuretics.
Anorexia and bulimia are serious eating disorders and can be fatal. The main similarity between the disorders is that both patients fear weight gain and use measures that are considered unhealthy or even dangerous to avoid obesity.
Both cases are often associated with mental disorders such as depression and anxiety disorders.
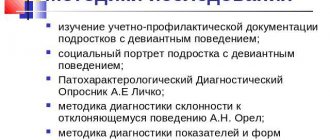
| anorexia | bulimia | |
| What is this | Eating disorders in which a person believes in and is overweight. For this reason, he chooses a low-calorie diet. | Eating disorders in which a person consumes high-calorie foods to avoid weight gain have harmful effects on health. |
| causes | There is no single cause, but cultural factors are the most common. | There are cases of genetic factors, but social factors such as stress and the need for beauty standards also contribute to the image. |
| symptoms | Body mass index is significantly below ideal. Physiological changes in the body. Anxiety and depression | The most common are induction of vomiting and the use of laxatives and diuretics. |
| treatment | Resumption of weight gain with medical and psychological monitoring | Therapy with continuation of therapeutic, nutritional and psychological tests. |
Eating disorders: how to get rid of anorexia and bulimia
Today I’m going to talk about the two main types of eating disorders: anorexia and bulimia, some of the nuances of their occurrence, all sorts of interesting numbers, and how you can cope with them. In general, the formation of anorexia and bulimia occurs easily. It is much more difficult and expensive to get rid of them later . I will tell you briefly, because everything that has been studied and written about these disorders cannot be summarized in one article. If you suspect you have an eating disorder, take the EAT-26 test for symptoms of anorexia and bulimia.
I want to say right away for meticulous readers - and this is correct! — I do not have a single “unsubstantiated” statement: all statistics and other figures used in the article are taken from literature not published on the Internet, namely from books and official booklets published by respected institutions. A list of references is attached at the end of the article.
Types of Eating Disorders
Eating disorders vary widely in severity and complexity, but two types stand out among them:
- bulimia nervosa
- anorexia nervosa
Quite simply, bulimia is when a person has the so-called. “binge episodes,” during which he eats an abnormally large amount of food; and after this attack, the person induces vomiting or uses laxatives in order to control weight and figure (although not always). Anorexia is when a person purposefully loses weight to the point of exhaustion and continues to consider himself “overweight” or “fat.” It happens when they are combined.
It is completely wrong to believe that the causes of these disorders are some kind of spoiledness, bad manners, weakness of will, “no one cooked them something tasty”, “if only they could at least once try a real Kiev cutlet...”, “we need to throw out the scales, yes and that’s all,” and so on. Unfortunately, everything is not that simple. Not at all like that.
These disorders are believed to only occur in women. No, that's not true either. The vast majority of people with anorexia or bulimia are women (up to 90%). And the remaining 10% are men.
Take a look at the chart: men are much more dissatisfied with their figure than women!
Minnesota experiment
American researchers from the University of Minnesota, USA, under the guidance of nutritionist and physiologist Ancel Keys, conducted the so-called. "Minnesota Fasting Experiment" , the results of which revolutionized the understanding of the influence of nutrition on the human psyche and on his physical health. About 40 specially selected and tested healthy men of different ages participated in this experiment. The experiment consisted of 3 stages:
- 3 months - normal nutrition and detailed analysis and recording of all manifestations, behavior, mood, etc.
- 6 months - food is reduced by half from the minimum required to maintain the weight of the participants. Recording all changes.
- 3 months - normal nutrition again.
The experiment had a huge impact on everyone involved, on the study of nutrition and on the psychology of eating behavior. There were both psychological and physiological consequences for the participants. We'll leave physiology for next time and concentrate on psychology.
Although there were significant differences between participants' individual experiences, overall, all male participants experienced dramatic physical, psychological and social changes as a result of food restriction. And besides, for many of them, the negative consequences continued even after their weight returned to their original weight, and the experiment had long ended .
One of the most impressive results of the Minnesota Experiment was that all participants changed their relationship with food . All noted that they found it difficult to concentrate on normal things and that they were constantly worried about thoughts about food and nutrition. Food became the main, if not the main, topic of their conversations, reading, dreams and dreams.
Some men became interested in cooking and began collecting recipes, while others became interested in kitchen tools. One participant in the experiment once found himself rummaging through a trash can to find something for his collection of kitchen tools. And, although the majority of men before the experiment were not at all interested in cooking and gastronomy, after the experiment, 40% of them reported that they were going to include food and its preparation in their future life plans . Some former participants in the experiment subsequently changed their career completely: they began working in the food industry.
The majority had serious psychological problems, incl. depression . One of the participants, being in some kind of “uncontrolled” state, amputated 3 fingers on his hand, and could not say whether he did it accidentally or intentionally. Other emotional problems included increased irritability, periodic outbursts of anger, and a sharp increase in anxiety . Some started smoking or biting their nails. Some people stopped taking care of their hygiene. Many had problems with thinking: concentration of attention, understanding, and ability to make decisions decreased. All participants, who previously spent 15-20 minutes eating, now sat over the plate for 1.5-2 hours, trying to make up for the lack of food with spices, tea, coffee and... chewing gum.
Almost all participants experienced a significant decrease in sexual interest , and also began to experience problems with communication . Some began to limit their communication with other people. Friendship, humor, plans for life, participation in some groups - all this faded into the background.
Some participants developed bulimic behavior - "binging and purging" - accompanied by very low mood, nausea and negative emotions such as self-loathing.
Within about a year after the end of the experiment, most returned to a normal diet. However, some, unfortunately, were never able to do this.
And all this as a result of restricting food by only half for 6 months. Many people currently suffering from anorexia and bulimia may restrict themselves by more than half of their diet for several years. And you say, “show him the cutlet and throw away the scales.”
Now, after such horrors, we move on to the current state of affairs. There will be no more horror stories, although it would take a very long time to list all the possible consequences from both the physical and psychological sides.
So what is bulimia?
There are studies that from 1% to 4% of all women will one way or another encounter bulimia or its manifestations in their lives. Bulimia is an eating disorder in which a person first eats a huge amount of food in fits and starts, after which he resorts to either laxatives or induces vomiting in order to control his weight. Initially, the weight of such people was either normal or slightly increased.
For example, during an attack of bulimia (about an hour), a woman, a housewife who is not overweight and of average height, can eat:
- 2 boxes of chocolates
- half a pack of cookies
- a glass of milk
- twelve sandwiches with butter
- two bananas
- one ice cream
- one jar of yogurt
- one pack of homemade cheese
Assess whether this is an objectively huge amount of food for this situation and this person?
Some professional areas can provoke a person to develop bulimia or anorexia: ballet, running, figure skating, modeling, gymnastics, bodybuilding, etc. That is, activities in which success is assessed based on body shape, figure and weight.
According to research, cognitive behavioral therapy is the most effective way to get rid of bulimia compared to other psychological interventions, and is better than pharmacotherapy (medicines) - cognitive behavioral therapy reduces the incidence of bulimia attacks by up to 85% (in those who have undergone therapy) . In addition, CBT reduces the risk of relapse.
There is a 2019 protocol called CBT-T . It is only suitable for those whose BMI is above 18 or a little lower. It should be very effective, but I can’t say anything yet - in my experience there is not enough for conclusions.
40% of patients are completely cured—they stop overeating and vomiting altogether. About 40% of patients show moderate results. However, within 10 years after the end of treatment, 89% of sufferers recover either completely or partially (17%) - this is due to the delayed effects of therapy, as well as the fact that patients begin to apply the methods in practice with greater success.
On average, a course of therapy for bulimia takes 4 to 5 months and includes 15 to 20 meetings with a psychotherapist.
And CBT-T , mentioned above, only includes 10 meetings maximum - provided that the client successfully completes the first 4, then it can be extended further. If he fails, it means it doesn’t work for him. The risk is higher, but there are also more benefits, both in terms of time, and in terms of money, and in terms of motivation.
How does a psychologist consult for bulimia:
- weight monitoring;
- regulation of nutrition, intervals and volumes of food;
- introduction of “forbidden foods” in order to prevent “bouts of gluttony”;
- learning specific ways to cope with problems;
- addressing dysfunctional beliefs about weight, shape, self, and body concept;
- if necessary, therapy for associated problems (usually depression);
- if necessary, consultations with other specialists: nutritionist, psychiatrist, therapist, etc.
- special training aimed at preventing relapses - because, unfortunately, this happens regardless of what therapy has been completed.
What is anorexia?
Anorexia is a disease that causes people to become extremely emaciated and yet believe that they are still overweight. The American Psychiatric Association estimates that on average 0.5 to 3.7% of all women will experience anorexia in their lifetime. In 90-95% of all cases of anorexia, the sufferers are women. As a rule, anorexia begins in adolescence when a girl who is slightly overweight or normal weight goes on a diet. Anorexia is a threat to life and health: up to 10% of those suffering from anorexia unfortunately die.
The causes of anorexia can be different:
- social pressure,
- "beauty standards"
- family environment,
- stressful situations
- cognitive disorders,
- biological factors (set weight, hypothalamic activity), etc.
The claim that diet alone causes anorexia is incorrect: most people who diet do not suffer from anorexia. However, in adolescent girls who strictly restrict themselves in nutrition, the likelihood of developing such a disorder during a year of strict diet increases by 18 times. A study was conducted in the USA that showed that anorexia is a disease of “white” women, African-American women have significantly different “ideals of female beauty” and are significantly more satisfied with their appearance.
At least half of those suffering from anorexia adhere to the “limiting food consumption” behavior model, that is, they have a clear list of foods that they do not consume: snacks, sweets, side dishes, flour, etc.
The main goal of anorexics is to lose weight. But at the same time, it is always based on fear: giving in to the desire to eat, becoming obese, losing control over weight. At the same time, being already objectively exhausted, depriving their body of important nutrients, these people, unfortunately, continue to follow their diet, becoming more and more concerned about the issue of nutrition.
Anorexia sufferers have various psychological problems. Anorexia is often accompanied by depression, low self-esteem, thoughts and assessments of oneself do not correspond to reality. Eating disorder sufferers also inaccurately perceive their body's internal signals: When anxious or upset, people with anorexia or bulimia often mistakenly think they are hungry - and react in the way they usually react to hunger - that is, by starting to eat. Take a look at the results of this interesting study conducted in the US in the 90s:
(Rebert, Stanton & Schwartz, 1991)
When do people eat junk food? Obviously, when they feel bad. People who experience positive emotions are more likely to eat normal food.
Treatment of anorexia
Treatment, or therapy, for anorexia should be comprehensive, with the involvement of specialists from various fields: nutritionists, psychiatrists, therapists, psychotherapists. In severe cases, hospitalization is carried out. According to foreign recommendations, treatment of anorexia should include, at a minimum:
- restoration of physical health damaged due to exhaustion;
- consultations with a nutritionist on nutrition issues in order to restore weight to an acceptable level;
- Cognitive behavioral therapy to help achieve and maintain an acceptable weight;
- family psychological therapy.
Up to 83% of those suffering from anorexia and who seek help successfully recover! However, relapses are possible a little later, and cognitive behavioral therapy helps to cope with them. Most people who recover subsequently find that they are happy to go to work, work efficiently, and form close relationships as often as other people.
Cognitive behavioral therapy can help anorexics work on co-occurring problems, such as depression, as well as irrational and dysfunctional beliefs, such as “I'm fat” or “No one likes me,” that contribute significantly to anorexic behavior. and low self-esteem.
Eating Attitude Test EAT-26 →
Literature:
- Comer, R. Pathopsychology of behavior. Mental disorders and pathologies. - St. Petersburg: Prime-Eurosign, 2007
- American Psychiatric Association. (2000). Practice guidelines for the treatment of patients with eating disorders (revision). American Journal of Psychiatry, 157(Suppl. 1), 1-39.
- Waller., G., Cordery H., Corstorphine E., Hinchichsen H., Lawson R., Mountford V., Russell K. (2007). Cognitive Behavioral Therapy for Eating Disorders. A Comprehensive Treatment Guide. Cambridge University Press.
- Fairburn, C. G. (2005). Evidence-based treatment of anorexia nervosa. International Journal of Eating Disorders, 37, S26-S30.
- National Institute of Clinical Excellence. (2004). Clinical guideline to Eating disorders – Quick reference guide.
- Center for Applied Research in Mental Health and Addictions (CARMHA) (2007). Cognitive Behavioral Therapy (Core Information).
- Agras, W. S., Walsh, T., Fairburn, C. G., Wilson, G. T., & Kraemer, H. C. (2000). A multicenter comparison of cognitive-behavioral therapy and interpersonal psychotherapy for bulimia nervosa. Archives of General Psychiatry, 57, 459-466.
- Wilson, G. T. (1999). Cognitive behavior therapy for eating disorders: Progress and problems. Behavior Research Therapy, Jul 37, Suppl.1:S79-95.
- McIntosh, V. V., Jordan, J., Carter, F. A., Luty, S. E., Mckenzie, J. M., Bulik, C. M., Frampton, C. M., & Joyce, P. R. (2005). Three psychotherapies for anorexia nervosa: A randomized, controlled trial. American Journal of Psychiatry, 162(4), 741-747.
- Wilson, G. T. (2005). Psychological treatment of eating disorders. Annual Review of Clinical Psychology, 1,439-465.
- Wilson, G. T., & Fairburn, C. G. (2002). Treatments for eating disorders. In P. E. Nathan & J. M. Gorman (Eds.). A guide to treatments that work (pp. 559-592). New York: Oxford University Press.
- Fairburn, C. G., & Bohn, K. (2005). Eating disorder NOS (EDNOS): An example of the troublesome “not otherwise specified” (NOS) category in DSM-IV. Behavioral Research and Therapy, 43, 691-701.
- Fairburn, C. G., & Harrison, P. J. (2003). Eating disorders. Lancet, 361,407-416.
- Moreno, M. A., & Judd, R. (2001). Eating disorder: Bulimia.eMedicine Journal, 2, 1-14.
- Vaz, F. J. (1998). Outcome of bulimia nervosa: Prognostic indicators. Journal of Psychosomatic Research, 45, 391-400.
- Fairburn, C. G., Norman, P. A., Welch, S. L., O'Connor, M. E., Doll, H. A., & Peveler, R. C. (1995). A prospective study of outcome in bulimia nervosa and the long-term effects of three psychological treatments. Archives of General Psychiatry, 52, 304-312.
- Pike K. M., Walsh B. T., Vitousek K., Wilson G. T., & Bauer J. (2003). Cognitive behavior therapy in the post-hospitalization treatment of anorexia nervosa. American Journal of Psychiatry, 160, 2046–2049.
- Thompson-Brenner, H., Glass, S., & Westen, D. (2003). A multidimensional meta-analysis of psychotherapy for bulimia nervosa. Clinical Psychology: Science and Practice, 10, 269-287.
- Steinhausen, H. C. (2002). The outcome of anorexia nervosa in the 20th century. American Journal of Psychiatry, 159, 1284–1293.
- Fairburn, C. G., Jones, R., Peveler, R. C., Hope, R. A., & O'Connor, M. (1993). Psychotherapy and bulimia nervosa. Longer-term effects ofinterpersonal psychotherapy, behavior therapy, and cognitive behavior therapy. Archives of General Psychiatry, 50, 419-428.
- American Psychiatric Association (2006). Practice Guideline for the Treatment of Patients With Eating Disorders (3rd edition - Eds. Joel Yager, Michael J. Devlin, Katherine A. Halmi, David B. Herzog, James E. Mitchell III, Pauline Powers, Kathryn J. Zerbe).
What is anorexia?
Anorexia nervosa is a disorder in which a person experiences excess weight. This happens even when he is within the normal weight range for height.
To achieve the goal of maintaining thinness (or even more weight loss), anorexics often deny the problem.
A person with anorexia eats little food or chooses low-calorie foods. And if he "loses control" and consumes high-calorie foods, he tends to resort to bulimia, another very common eating disorder among people with anorexia.
Types of anorexia
As mentioned above, anorexia is rarely the only diagnosis. Very often, in parallel, the patient suffers from other disorders. From a psychological point of view, anorexia is classified as follows:
- Primary anorexia is diagnosed in children under 10-12 years of age. As a rule, they lose their appetite for psychological reasons - conflicts in the family and at school, parental divorce, death of a loved one or pet. Such traumas can leave a deep imprint on a child’s psyche, even if the child does not admit it. The worst thing a parent can do in such a situation is to force-feed the child. As a result, anorexia can take on the form of behavior “in spite”, when the child withdraws into himself and generally refuses to make contact with adults and psychologists.
- Anorexia nervosa syndrome, in which the patient loses 15-60 percent of body weight in a short period of time. Anorexia nervosa occurs in both adolescents and adults. Moreover, in some clinical cases, a person does not seek to lose weight, he simply loses his appetite as a result of the trauma he has experienced. Anorexia nervosa may not have a uniform course: acute periods are followed by remission. During remission, the patient can regain some of his body weight, but after a while a relapse occurs again. In psychology, anorexia nervosa often goes “hand in hand” with a post-stress period, increased anxiety, depressive disorders, and body dysmorphic disorder.
- Drug-induced anorexia usually occurs unconsciously. As a result of taking certain medications, the patient loses appetite and interest in food, his eating behavior changes unnoticed by others and himself. With drug-induced anorexia, it is usually enough to simply stop taking the medications that caused the loss of interest in food.
- A relatively rare type of eating disorder is male anorexia. The psychology of men is structured differently than that of women. Representatives of the stronger sex are not characterized by dysmorphophobia and the desire to lose weight. Typically, male anorexia is caused by post-traumatic stress disorder. Often representatives of the stronger sex do not sufficiently reflect a decrease in appetite. Relatives and loved ones begin to sound the alarm when significant body weight has already been lost.
Causes of anorexia
Scientists have not yet reached a consensus on the origins of anorexia, but like genetic factors, cultural factors may be associated with the development of the disease. This is because societies where thinness is valued have higher incidences of anorexia.
Anxiety and depression may also be associated with the disorder. Again, both qualities can be acquired if thinness is the most acceptable standard and excess weight is doomed, creating a vicious circle that can lead to anorexia.
Symptoms of anorexia
In general, a person with anorexia will have a body mass index of less than 18. This means that they are very light for their height and age. Continuous weight loss is another symptom.
Additionally, a person with anorexia may have lower libido levels. Some women even stop menstrual cycles due to illness.
If episodes of anorexia occur during an individual's growth phase, the disease can cause severe damage or impairment to skeletal and muscular development.
Anxiety and depression, although they are symptoms of various medical conditions, can also be signs of anorexia, especially if they are too mild.
Treatment of anorexia
First of all, a person needs to gain weight in order for the body to become healthy again. This is because in extreme cases of anorexia nervosa, patients can lose so much weight that secondary problems such as osteoporosis and infertility can occur.
This is why restoring a healthy weight is so important for anorexia patients. Additionally, treating anxiety and depression helps a person cope with the disease.
It is also extremely important that they have psychological counseling. Although most people only have one bout of anorexia in their lives, some cases can recur and, if not treated properly, can become a lifelong problem.
What is bulimia?
Bulimia, also known as bulimia nervosa, is an eating disorder. It is characterized by a person's urge to eat food (usually high in calories) and immediately use measures to prevent weight gain, such as inducing vomiting and using laxatives and diuretics.
As with anorexia, a thin person with bulimia perceives themselves as fat, even if they are within the normal body weight range. For this reason, it is also associated with mental disorders that could occur in childhood and even throughout life.
Causes of bulimia
Scientists agree that genetic factors account for 30% to 80% of bulimia cases. However, mental stress, cultural pressure on beauty standards, obesity and lack of self-esteem can also cause bulimia.
A person with anorexia can also practice to prevent weight gain. In this sense, anxiety and depression also pose a risk for developing bulimia.
Another risk factor, especially for children and adolescents, is living in a family that enforces frequent dieting and excess weight.
Reasons for the development of anorexia
Depending on the stage and concomitant diseases, treatment is prescribed. One symptom of anorexia nervosa can be identified, the most obvious one being lack of appetite. The reasons for the development of the disorder are as follows:
- In psychology there is such a thing as the theory of phobic food avoidance. The girl dreams of losing weight, it becomes her obsession. As a result, she develops anorexia and eventually stops feeling hungry. In the absence of adequate comprehensive treatment, death can occur.
- Disharmonious teenage crisis - often teenage girls suffer from a discrepancy between reality and their expectations from it. As a result, they lose their appetite, exhaustion develops, and other mental disorders appear in parallel. If the reason is a crisis, then you should find a good psychologist or psychotherapist to work with the teenager. In most cases, concurrent drug therapy is necessary.
- Personal factors - pedantic, neurotic individuals often try to achieve, from their point of view, an ideal figure. The result is borderline disorder. As a rule, in this case, obsessive-compulsive disorder, a neurotic condition, can be diagnosed in parallel with anorexia.
- Cultural factors - the desire to look as thin as possible, imitating one's own fictitious ideal (celebrities, models, etc.). In this case, we can talk about dysmorphophobia, that is, dissatisfaction with one’s own body and appearance, which is accompanied by anorexia. In psychology, the cause of dissatisfaction with one's own appearance is interpreted as a consequence of childhood or adolescent trauma. A person can bring himself to complete exhaustion just in order to meet some illusory fictional ideals.
Treatment for bulimia
Although many patients do not see the need for treatment because they do not believe they have an eating disorder, in the case of bulimia, cognitive behavioral therapy is the main treatment option.
However, psychological, psychiatric and nutritional monitoring is necessary. Some antidepressants may be indicated, but only in extreme cases. Mood stabilizers may also be prescribed.
However, it is very important for a person to understand his emotions and feelings in relation to his body. Therefore, we are dealing with anxiety and depression, which are factors behind the development of the disorder
Psychotherapeutic treatment of anorexia nervosa
I do not work with anorexia because it is a life-threatening disease that requires teamwork of specialists. Sometimes the client also has to go to the hospital. I have neither a team nor a hospital - and I always redirect everyone who comes with this diagnosis to the right places for treatment.
With the exception of very rare cases, when the BMI has been consistently above 18 for a long time and does not fall during therapy, and blood tests do not threaten a lack of substances. I'm watching