All possible causes of mental retardation
Manifestations of mental retardation in an adult may appear due to socio-psychological pressure, and in children due to biological factors that lead to immediate developmental delay. Biological causes include: disruptions (damage) of the central nervous system, residual effects due to damage. A sick child may be born if during pregnancy:
- Rhesus conflict was determined;
- persistent and severe toxicosis was observed;
- doctors discovered intrauterine infections;
- fetal hypoxia occurred.
Children who were born prematurely or received skull injuries during childbirth are at risk. Also, with kernicterus, there is a risk of developing cervical development in adulthood. Even if the baby was born healthy, there is a possibility of developmental delay in the future due to somatic diseases:
- abnormal bone development;
- malnutrition;
- infections affecting the nervous system;
- flu;
- epilepsy attacks
- serious injuries to the skull and brain.
Social factors are very important and can affect a child's well-being. If a teenager feels excessive care or indifference on the part of his parents, he is raised by despotic methods, or there is a lack of communication with other people, then problems may arise. Mental retardation in adults often occurs due to dysfunction of the organs of vision, hearing, and speech apparatus.
Article on the topic: Symptoms and signs of mental retardation in children
Classifications
In studies conducted in 1972-1973. Research Institute of Defectology of the Academy of Pedagogical Sciences of the USSR in a number of cities and rural areas of the USSR (Moscow, Irkutsk region, Lithuania, Armenia), 5.8% of all primary school students were diagnosed with mental retardation. Based on the materials of these studies, M. S. Pevzner and T. A. Vlasova proposed dividing the general group of ZPR into two types.
- Uncomplicated psychophysical and mental infantilism
- “Secondary” mental retardation, caused by persistent cerebrovascular disease (increased exhaustion of mental functions) of various origins, which arose in the early stages of ontogenesis, and therefore cognitive activity and performance are primarily impaired.
Subsequently, based on this classification, K. S. Lebedinskaya proposed a classification according to the etiopathogenetic principle: [1]
- ZPR of constitutional origin (uncomplicated mental and psychophysical infantilism, according to the classification of M. S. Pevzner and T. A. Vlasova). “We are talking about the so-called harmonious infantilism, in which the emotional-volitional sphere is, as it were, at an earlier stage of development, in many ways reminiscent of the normal structure of the emotional makeup of younger children.”[2] Such children are characterized by bright, but superficial and unstable emotions, a predominance of play motivation, heightened mood, and spontaneity. Difficulties in learning in the early grades are associated with the predominance of play motivation over cognitive motivation, immaturity of the emotional-volitional sphere and the personality as a whole. In such cases, all the qualities described above are often combined with an infantile body type (gracefulness). This combination of mental and physical traits is often caused by hereditary factors, which makes it possible to see in it one of the types of normative psychophysical development (A.F. Melnikova, 1936; G.E. Sukhareva, 1965). Sometimes it is also associated with the characteristics of intrauterine development, in particular, multiple births (G. P. Bertyn (1970) on the relative frequency of harmonic infantilism in twins)
- ZPR of somatogenic origin. This type of mental retardation is due to the influence of various severe somatic conditions suffered at an early age (surgeries with anesthesia, heart disease, low mobility, asthenic conditions). “There is often a delay in emotional development - somatogenic infantilism, caused by a number of neurotic layers - uncertainty, timidity, capriciousness associated with a feeling of physical inferiority" [2]
- ZPR of psychogenic origin. This type of disorder is associated with unfavorable upbringing conditions that arose early and lasted for a long time. This type of mental retardation occurs in three main cases: Insufficient care, neglect. This is the most common option. In such cases, the child experiences abnormal personality development of the type of mental instability (G. E. Sukhareva, 1959; V. V. Kovalev, 1979, etc.). The child does not develop forms of behavior associated with active inhibition of affect. The development of cognitive activity and intellectual interests is not stimulated. Features of immaturity of the emotional-volitional sphere are observed, namely: affective lability, impulsiveness, increased suggestibility. There is also a lack of basic knowledge and understanding necessary for mastering the school curriculum. Lebedinskaya separately notes that this type of mental retardation should be distinguished from the phenomena of pedagogical neglect, which are not a pathological phenomenon, but a limited deficit of knowledge and skills due to a lack of intellectual information.
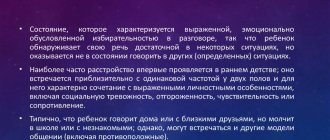
- Hyperprotection, or upbringing according to the “family idol” type. Most often occurs in anxious parents. They “tie” the child to themselves, simultaneously indulging the child’s whims and forcing him to act in the most convenient and safe way for the parent. Any obstacles or dangers, both real and imaginary, are removed from the child’s environment. Thus, the child is deprived of the opportunity to independently overcome difficulties, to correlate his desires and needs with the efforts that must be made to realize them, as a result, the same inability to inhibit his own affect, emotional lability, etc. arises. The child is not independent, not initiative, self-centered, incapable of sustained volitional effort, overly dependent on adults. Personality development follows the principle of psychogenic infantilism.
- Personality development according to the neurotic type. It is observed in families with very authoritarian parents or where constant physical violence, rudeness, despoticism, aggression towards the child and other family members are allowed. The child may experience obsessions, neuroses or neurosis-like conditions. An emotionally immature personality is formed, which is characterized by fears, an increased level of anxiety, indecision, lack of initiative, and a possible syndrome of learned helplessness. The intellectual sphere suffers, since all the child’s activities are subordinated to the motive of avoiding failure, and not achieving success, therefore, such children, in principle, will not do anything that could once again confirm their failure.
The classification of V.V. Kovalev (1979) is also interesting. He identifies four variants of PPD, caused by the influence of biological factors:
- Dysontogenetic (with mental infantilism);
- Encephalopathic (with mild organic lesions of the central nervous system);
- Mental retardation of a secondary nature with sensory defects (with early visual and hearing impairments),
- ZPR associated with early social deprivation (for example, during hospitalization).
Classification of ZPR
The famous defectologist and psychiatrist Klara Lebedinskaya in her works explained whether mental retardation occurs in adults, and created a classification of the disease that doctors use.
- The constitutional type of the disease indicates delayed maturation of the central nervous system. At the same time, infantilism is harmonious. If this type of disease is diagnosed, the patient will behave like a child. The behavior of people with mental retardation does not correspond to the chronological age group. They have insufficient concentration, slow mental activity, and are spontaneity and unpredictability. Even at an older age, they want to play, do something simple and understandable.
- With psychogenic genesis, it is worth talking about the social conditions in which the person lived. It is because of abuse, lack of attention, and overprotection that symptoms of mental retardation in an adult are observed. Lack of parental attention has a negative impact on the psyche: the child becomes impulsive, withdrawn, aggressive, and has no desire or desire to learn anything new. With overprotection, there is a reluctance to do anything, lethargy, and apathy.
- The cerebral-organic type of developmental delay is primary and is associated with brain injury. Then cognitive activity cannot be fully formed. Such people most often look “inhibited” and not emotional.
- Somatogenic genesis will lead to the consequences of mental retardation in adulthood. In the medical history of patients, along with somatogenic delay in the development of mental health, one can find diagnoses: pneumonia, renal failure, asthma, bronchitis and others. Adults with this disease have low performance, superficial attention, and get tired quickly. Due to poorly developed skills, they cannot find a good job or start a family.
Symptoms of mental retardation in adults
- isolation and detachment;
- indecision;
- attacks of panic and anxiety;
- aggressive behavior;
- stuttering;
- dyslalia;
- mental retardation;
- uncontrolled facial expressions and others.
The final diagnosis is made after diagnosing the whole body and consulting with highly specialized doctors. It is determined by the Psychological, Medical and Pedagogical Commission (PMPC). It consists of a speech therapist, psychologist, psychiatrist and other specialists.
Who carries out the diagnosis and when?
A commission diagnoses mental retardation in the child. Composition: psychologist, neurologist, teacher, psychiatrist, speech therapist, defectologist. During the diagnosis, parents, representatives of the kindergarten or school are present. Their task includes:
- Give a conclusion or reject the diagnosis of mental retardation.
- The child is tested on his knowledge. They check reading, writing, counting, logic, and the child answers certain tests.
- Experts study the child’s perception, memory, thinking, attentiveness, and self-awareness.
- The commission establishes the training program and what specific classes are needed.
Preschoolers up to 6 years old are diagnosed. Additionally, the doctor may prescribe an EEG, MRI, or CT scan of the brain.
The essence of diagnosis and correction
If the diagnosis has already been made, then you need to be periodically examined and consult with specialists. To stage it, it is necessary to collect and provide doctors with a medical history, talk about the patient’s living conditions, and personal observations. Neuropsychological testing and examinations of the speech apparatus are mandatory.
Doctors talk with the patient, examine his intellectual abilities, emotional and volitional qualities. An electrocardiogram, computed tomography, and magnetic resonance imaging are performed. According to the results of tests and diagnosis of PMPK, the doctor makes a decision and gives recommendations to parents.
Doctors can diagnose the disease from an early age, after which the person will face the symptoms and manifestations of the disease throughout his life. With the help of proper correction, it will be possible to alleviate the patient’s condition and help him live a full life.
Medical support for the correction of the disease begins from the moment of diagnosis until complete recovery (if doctors give a positive prognosis). Children go to specialized educational institutions or classes and study according to a special program. Play therapy and art therapy are the best methods to help teenagers with mental retardation. Drug treatment is also used for the somatic genesis of the disease.
Article on the topic: Symptoms and signs of hyperactivity in adults
Methods for correcting mental retardation
In a difficult situation, first of all, you should not despair. Delays in the development of a child’s psyche are not a death sentence, but only a reason for serious treatment. There are quite frequent cases when such children study in regular secondary schools and do well in all subjects.
On the other hand, teachers and parents must understand that the difficulties that a child has every day with understanding subjects, learning and the ability to remember what he has learned are not at all the result of his laziness or pathological depravity.
You should not constantly scold your child for negligence and scold him for negative aspects in learning, but on the contrary, support him and treat him with special attention, showing understanding.
It is possible to apply an individual approach to each of the difficult children, taking into account the nature, characteristics of upbringing and the causes of such a disease. If parents are able, it is better to hire a tutor for him and organize classes with a teacher of the deaf – a specialist in children’s learning problems. In particularly difficult cases, doctors prescribe medication.
User comments
Adults with mental retardation can live a normal life if their parents began to deal with their problem from an early age. Netizens shared their opinions about treatment and correction of the disease. They talked about how their sick children lived. Materials were taken from https://www.baby.ru/community/view/126532/forum/post/617898024/ https://www.baby.ru/community/view/126532/forum/post/617898024/ and others Internet platforms.
Life of people with mental retardation
| Positive reviews | Negative reviews |
| I was interested in the consequences of mental retardation in adulthood, so I went to the forum. My child was diagnosed with mental retardation. Corrective and medicinal treatment was prescribed. After 2 years, I managed to achieve good results, but there is still a fear that the symptoms of the disease may reappear. | PMPK only puts a mark on the child. We were diagnosed with developmental delay. This was followed by work with a defectologist and psychologist. We also went for massages and physiotherapy. There is very little effectiveness from manipulation and working with specialists. |
| My son was diagnosed at age 4, and work with a speech therapist began. Within 2 years the child began to speak like a 4-5 year old. Doctors are convinced that this is a positive result of therapy. I will send him to a special class at school so that he does not feel mentally retarded. | I am categorically against my Sasha, who has mental retardation, being sent to a separate class for inclusive education. He will be among other sick children, so he will not be able to adapt and will not strive to learn something new. |
| We have inclusive classes for children in our city (they recently opened). Unfortunately, the neighbors encountered a problem - the child has a mental disorder. He has already grown up, the symptoms remain a little, but he lives a normal life, even got a job. | An acquaintance has an adult son and he has been living with mental retardation for more than 15 years. The illness hinders him in absolutely everything: no friends, no beloved, no job. Only online communication. It turns out that his parents will have to look after him throughout his life. |
| I have a daughter, she is now 19 years old. She lives with inhibited mental development for a long period of time. However, she graduated from school and is now studying in absentia at a university. Everything is possible, there is no need to give up on children. If you get treatment and take care of your child, everything will return to normal. | Adults who have completed their mental health program are not hired, and if they are hired, it is for low-paid positions. It is very difficult to live with such a diagnosis. |
| I am a tiler and I have 2 colleagues who are deaf and mute. They were hired. Recently a guy with a mental disorder came in and was hired as well. If you have the desire, then everything will work out. | With mental retardation, adults cannot always organize their lives. What kind of work can we talk about if the patient cannot even set an alarm clock so as not to oversleep? You also need to do quality work and adhere to discipline, which people with mental retardation cannot do. |
| There are many correction programs in Moscow that really help. Good doctors got the child back on his feet. The girl is now 17 years old. She behaves quite normally, her speech defects are completely gone. We are grateful to the doctors. | Each person has a different course of development. Doctors said that my over-aged son with this diagnosis would need my constant care. He is 21 years old, he will not work or help his family. It's terrible to realize this. Of course, you want only the best for your child, but when you don’t see any improvement during treatment, you give up. |
| Now the quality of medicine has improved, many innovative techniques have appeared. Also, the specialists know their business. During therapy (3 years of treatment) it was possible to minimize the symptoms. We are still working with a speech therapist. Doctors said that with age, symptoms may decrease, which is what happened in our case. I recommend that mothers observe their sons’ and daughters’ behavioral decisions, speech, and intellectual abilities from early childhood. | If a person has an unstable emotional state, he will not be able to work. This is why people with mental disabilities cannot find employment. |
Features of children with mental retardation educational and methodological material
“Features of teaching children with mental retardation”
Speech at the pedagogical council in a general education institution
Prepared by: Chernoyarova N.S., primary school teacher.
Among students experiencing persistent difficulties in learning and adapting to school, a special place is occupied by children who do not have pronounced sensory deviations, as well as gross impairments of intellectual and speech development - these are schoolchildren with mental retardation who are studying under a correctional program.
Concept and classification of mental retardation
In its modern meaning, the term “mental retardation” refers to syndromes of temporary lag in the development of the psyche as a whole or its individual functions (motor, sensory, speech, emotional-volitional). In other words, this is a state of slow pace of realization of the body’s properties encoded in the genotype due to temporarily and mildly acting factors (for example, poor care, etc.).
Delayed mental development may be due to the following reasons:
- socio-pedagogical (lack of parental care, normal conditions for teaching and raising children, pedagogical neglect, the child being in a difficult life situation);
- physiological (severe infectious diseases, traumatic brain injuries, hereditary predisposition, etc.) There are two main forms of mental retardation:
- delayed mental development caused by mental and psychophysical infantilism, where the main place is occupied by underdevelopment of the emotional-volitional sphere;
- developmental delay that occurs in the early stages of a child’s life and is caused by long-term asthenic and cerebrasthenic conditions.
Delayed mental development in the form of uncomplicated mental infantilism is considered more favorable than in cerebrasthenic disorders, when not only long-term psychological correction work is necessary, but also therapeutic measures.
There are four main options for ZPR:
1) mental retardation of constitutional origin;
2) mental retardation of somatogenic origin;
3) mental retardation of psychogenic origin;
4) mental retardation of cerebral-organic origin.
In the clinical and psychological structure of each of the listed options for mental retardation, there is a specific combination of immaturity in the emotional-volitional and intellectual spheres.
1. ZPR of constitutional origin.
Causes: metabolic disorders, genotype specificity.
Symptoms: delayed physical development, development of static-dynamic psychomotor functions; intellectual impairments, emotional and personal immaturity, manifested in affects, behavioral disorders.
2. ZPR of somatogenic origin.
Causes: long-term somatic diseases, infections, allergies.
Symptoms: delayed psychomotor and speech development; intellectual disabilities; neuropathic disorders, expressed in isolation, timidity, shyness, low self-esteem, lack of development of children's competence; emotional immaturity.
3. Mental retardation of psychogenic origin.
Reasons: unfavorable upbringing conditions in the early stages of ontogenesis, traumatic microenvironment.
Symptoms: lack of development of children's competence and voluntary regulation of activity and behavior; pathological personality development; emotional disorders.
4. ZPR of cerebral-organic origin.
Causes: point organic damage to the central nervous system of a residual nature, due to the pathology of pregnancy and childbirth, trauma to the central nervous system and intoxication.
Symptoms: delayed psychomotor development, intellectual impairment, organic infantilism.
Symptoms: delayed psychomotor development, intellectual impairment, organic infantilism.
Children with mental retardation of cerebral-organic origin are the most difficult in diagnostic terms, because, like children with mental retardation, they consistently fail in the first years of education.
Depending on the origin (cerebral, constitutional, somatic, psychogenic), and the time of exposure of the child’s body to harmful factors, mental retardation gives rise to different types of deviations in the emotional-volitional sphere and cognitive activity.
As a result of the study of mental processes in children with mental retardation, a number of specific features were identified in their cognitive, emotional-volitional activity, behavior and personality in general, characteristic of the majority of children in this category.
Numerous studies have established the following main features of children with mental retardation: increased exhaustion and, as a result, low performance; immaturity of emotions, will, behavior; limited supply of general information and ideas; poor vocabulary, lack of intellectual skills; gaming activity is also not fully formed. Perception is characterized by slowness. Difficulties in verbal and logical operations are revealed in thinking. Children with mental retardation suffer from all types of memory and lack the ability to use aids for memorization. They need a longer period to receive and process information.
In persistent forms of mental retardation of cerebral-organic origin, in addition to disorders of cognitive activity caused by impaired performance, insufficient formation of certain cortical or subcortical functions is often observed: auditory, visual perception, spatial synthesis, motor and sensory aspects of speech, long-term and short-term memory.
Thus, along with general features, children with variants of mental retardation of various clinical etiologies are characterized by characteristic features, the need to take them into account in psychological research, during training and correctional work is obvious.
Psychological characteristics of children with mental retardation in educational activities
Experts who study the psychological patterns of development of this category of children indicate that psychological and pedagogical study reveals a number of features that distinguish them from mentally retarded children. They solve many practical and intellectual problems at the level of their age, are able to take advantage of the assistance provided, are able to comprehend the plot of a picture or story, understand the conditions of a simple task and perform many other tasks. At the same time, these students have insufficient cognitive activity, which, combined with rapid fatigue and exhaustion, can seriously hamper their learning and development. Rapidly onset fatigue leads to loss of performance, as a result of which students have difficulties in mastering educational material: they do not retain the terms of the task or a dictated sentence in their memory, and forget words; make ridiculous mistakes in written work; often, instead of solving a problem, they simply mechanically manipulate numbers; find themselves unable to evaluate the results of their actions; their ideas about the world around them are not broad enough.
Children with mental retardation cannot concentrate on a task and do not know how to subordinate their actions to rules containing several conditions. Many of them are dominated by gaming motives.
It is noted that sometimes such children actively work in the classroom and complete tasks together with all the students, but soon get tired, begin to get distracted, and stop perceiving the educational material, resulting in significant gaps in knowledge.
Thus, reduced activity of mental activity, insufficient processes of analysis, synthesis, comparison, generalization, weakened memory, attention do not go unnoticed, and teachers try to provide each of these children with individual assistance: they try to identify gaps in their knowledge and fill them in one way or another – explain the educational material again and give additional exercises; more often than when working with normally developing children, visual teaching aids and a variety of cards are used to help the child concentrate on the main material of the lesson and free him from work that is not directly related to the topic being studied; organize the attention of such children in different ways and attract them to work.
All these measures at individual stages of learning certainly lead to positive results and allow one to achieve temporary success, which allows the teacher to consider the student not as mentally retarded, but only as a developmentally delayed one who is slow to assimilate educational material.
During periods of normal performance, children with mental retardation exhibit a number of positive aspects of their activity, characterizing the preservation of many personal and intellectual qualities. These strengths most often manifest themselves when children perform accessible and interesting tasks that do not require prolonged mental stress and take place in a calm, friendly environment.
In this state, when working individually with them, children are able to independently or with little help solve intellectual problems almost at the level of normally developing peers (group objects, establish cause-and-effect relationships in stories with hidden meanings, understand the figurative meaning of proverbs).
A similar picture is observed in the classroom. Children can relatively quickly understand educational material, perform exercises correctly and, guided by the image or purpose of the task, correct mistakes in their work.
By the 3rd–4th grade, some children with mental retardation develop an interest in reading under the influence of the work of teachers and educators. In a state of relatively good performance, many of them consistently and in detail retell the available text, correctly answer questions about what they read, and are able, with the help of an adult, to highlight the main thing in it; Stories that are interesting to children often evoke strong and deep emotional reactions in them.
In extracurricular life, children are usually active; their interests, like those of normally developing children, are varied. Some of them prefer quiet, calm activities: modeling, drawing, design, and enthusiastically work with building materials and cut-out pictures. But such children are in the minority. Most prefer outdoor games, like to run and frolic. Unfortunately, both “quiet” and “noisy” children tend to have little imagination and invention in independent games.
All children with mental retardation love various kinds of excursions, visiting theatres, cinemas and museums, sometimes it captivates them so much that they are impressed by what they see for several days. They also love physical education and sports games, and although they exhibit obvious motor clumsiness, lack of coordination of movements, and inability to obey a given (musical or verbal) rhythm, over time, in the learning process, schoolchildren achieve significant success and in this regard compare favorably from mentally retarded children.
Children with mental retardation value the trust of adults, but this does not save them from breakdowns, which often occur against their will and consciousness, without sufficient grounds. Then they have difficulty coming to their senses and feel awkward and depressed for a long time.
The described features of the behavior of children with mental retardation, when not sufficiently familiar with them (for example, during a one-time lesson visit), can create the impression that all the conditions and learning requirements provided for students in a general education school are quite applicable to them. However, a comprehensive (clinical and psychological-pedagogical) study of students in this category shows that this is far from the case. Their psychophysiological characteristics, the uniqueness of cognitive activity and behavior lead to the fact that the content and methods of teaching, the pace of work and the requirements of a comprehensive school are beyond their strength.
The working state of children with mental retardation, during which they are able to master educational material and correctly solve certain problems, is short-lived. As teachers note, children are often able to work in class for only 15–20 minutes, and then fatigue and exhaustion set in, interest in classes disappears, and work stops. In a state of fatigue, their attention sharply decreases, impulsive, thoughtless actions occur, and many errors and corrections appear in their work. For some children, their own powerlessness causes irritation, while others categorically refuse to work, especially if they need to learn new educational material.
This small amount of knowledge, which children manage to acquire during the period of normal performance, seems to hang in the air, is not connected with subsequent material, and is not sufficiently consolidated. Knowledge in many cases remains incomplete, fragmentary, and not systematized. Following this, children develop extreme self-doubt and dissatisfaction with educational activities. When working independently, children get lost, begin to get nervous, and then cannot complete even basic tasks. Severe fatigue occurs after activities that require intense mental expression.
In general, children with mental retardation gravitate towards mechanical work that does not require mental effort: filling out ready-made forms, making simple crafts, composing problems based on a model with only subject and numerical data changed. They have difficulty switching from one type of activity to another:
Having completed the example on division, they often carry out the same operation in the next task, although it is on multiplication. Monotonous actions, not mechanical, but associated with mental stress, also quickly tire students.
At the age of 7–8 years, such students have a hard time getting into the working mode of the lesson. For a long time, the lesson remains a game for them, so they can jump up, walk around the class, talk with their friends, shout something, ask questions not related to the lesson, endlessly ask the teacher again. When children get tired, they begin to behave differently: some become lethargic and passive, lie down on their desks, look aimlessly out the window, become quiet, do not annoy the teacher, but also do not work. In their free time, they tend to retire and hide from their comrades. Others, on the contrary, experience increased excitability, disinhibition, and motor restlessness. They are constantly twirling something in their hands, fiddling with the buttons on their suit, playing with different objects. These children, as a rule, are very touchy and hot-tempered, often without sufficient reason they can be rude, offend a friend, and sometimes become cruel.
Bringing children out of such states requires time, special methods and great tact on the part of the teacher.
Realizing their difficulties in learning, some students try to assert themselves in their own ways: they subjugate their physically weaker comrades, command them, force them to do unpleasant work for themselves (cleaning the classroom), show their “heroism” by performing risky actions (jumping from a height, climbing along dangerous stairs, etc.); They can tell lies, for example, boast about some actions that they did not commit. At the same time, these children are usually sensitive to unfair accusations, react sharply to them, and have difficulty calming down. Physically weaker schoolchildren easily obey “authorities” and can support their “leaders” even when they are clearly wrong.
Incorrect behavior, which manifests itself in relatively harmless acts in younger schoolchildren, can develop into persistent character traits if appropriate educational measures are not taken in a timely manner.
Knowledge of the developmental characteristics of children with mental retardation is extremely important for understanding the general approach to working with them.
Principles of correctional and developmental education for children with mental retardation
The psychological characteristics of children with mental retardation lead to their failure at school. The knowledge acquired by students with mental retardation in a general education school does not meet the requirements of the school curriculum. Particularly poorly mastered (or not mastered at all) are those sections of the program that require significant mental work or consistent multi-stage establishment of relationships between the objects or phenomena being studied. Consequently, the principle of systematic learning, which provides for children with mental retardation to master the fundamentals of science in the form of a system of knowledge, skills and abilities, remains unrealized. The principle of consciousness and activity in learning remains equally unrealized for them. Children often memorize certain rules, regulations, laws mechanically and therefore cannot apply them when working independently.
When performing written work, mistakes in the actions necessary for the correct completion of the task, which are very typical for children in this category, are revealed. This is evidenced by the numerous corrections made by the child as he works, the large number of errors that remain uncorrected, the frequent violation of the sequence of actions and the omission of individual parts of the task. Such shortcomings in many cases can be explained by the impulsiveness of such students and the insufficient development of their activities.
The low level of educational knowledge serves as evidence of the low productivity of education of children of this group in a comprehensive school. But the search for effective teaching tools must be carried out not only in connection with the development of techniques and methods of work that are adequate to the developmental characteristics of such children. The content of training itself should acquire a correctional orientation.
It is known that a normally developing child begins to master mental operations and methods of mental activity already in preschool age. The lack of formation of these operations and methods of action in children with mental retardation leads to the fact that even at school age they find themselves tied to a specific situation, due to which the acquired knowledge remains scattered and is often limited to direct sensory experience. Such knowledge does not ensure the full development of children. Only when brought into a single logical system do they become the basis for the student’s mental growth and a means of activating cognitive activity.
An integral part of remedial education for children with mental retardation is the normalization of their activities, and in particular educational activities, which are characterized by extreme disorganization, impulsiveness, and low productivity. Students in this category do not know how to plan their actions and control them; They are not guided in their activities by the ultimate goal, they often “jump” from one thing to another without completing what they started.
Impaired activity in children with mental retardation is a significant component in the structure of the defect; it inhibits the child’s learning and development. Normalization of activity is an important part of the correctional education of such children, which is carried out in all lessons and outside of school hours, but overcoming some aspects of this disorder may be the content of special classes.
Thus, a number of characteristics of children with mental retardation determine the general approach to the child, the specifics of the content and methods of correctional education. Subject to specific learning conditions, children in this category are able to master educational material of considerable complexity, designed for normally developing students in general education schools. This is confirmed by the experience of teaching children in special classes and the success of the subsequent education of most of them in general education schools.
conclusions
When mental development is delayed, there is insufficiency of the central nervous system, leading to uneven formation of mental functions, which determines the characteristics of development and behavior of children and determines the specifics of the content and methods of correctional education.
The psychological and pedagogical characteristics of children with mental retardation include distinctive features of this category of children both from normally developing peers and from children with mental retardation. However, due to the similarity of behavioral manifestations, differential diagnosis can present certain difficulties. A comprehensive psychological examination and study of the cognitive activity of children with mental retardation are an important factor in the correct diagnosis and choice of ways of training and correction.
By the beginning of school, these children, as a rule, have not formed the basic mental operations - analysis, synthesis, comparison, generalization. They do not know how to navigate a task, do not plan their activities, but unlike the mentally retarded, they have higher learning ability, they use help better and are able to transfer the shown method of action to a similar task.
Subject to specific learning conditions, children in this category are able to master educational material of considerable complexity, designed for normally developing students in general education schools.
Conclusion
Adults may experience symptoms and signs of mental retardation that were diagnosed in early childhood for certain reasons. As the patient grows older, his condition may improve or worsen, but working with qualified doctors will help cope with speech defects, improve brain activity and motor skills.
If you contact professionals in a timely manner, an individual program will be developed and therapies will be offered that will help you lead a normal life in adulthood.